S-ar putea să vă placă și
- North Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaDe la EverandNorth Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaErica C. BjornstadÎncă nu există evaluări
- Name: Mrs. N.S. Age: 20 Yo Address: Narmada Admitted: October, 29 2012 at 10.30 WitaDocument6 paginiName: Mrs. N.S. Age: 20 Yo Address: Narmada Admitted: October, 29 2012 at 10.30 WitaLaili KhairaniÎncă nu există evaluări
- MR OBGYN 14 Okt 2012 - KPD - SCDocument10 paginiMR OBGYN 14 Okt 2012 - KPD - SCPutra MahautamaÎncă nu există evaluări
- Morning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsDocument8 paginiMorning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsEra MoetzÎncă nu există evaluări
- MR 13agustus13 - KPD Preterm Drip MRDocument11 paginiMR 13agustus13 - KPD Preterm Drip MRIda Andalos TothaÎncă nu există evaluări
- Supervisor: Dr. Gede Made Punarbawa, SP - OG (K) Medical Students: TiaDocument10 paginiSupervisor: Dr. Gede Made Punarbawa, SP - OG (K) Medical Students: TiaRian Segal HidajatÎncă nu există evaluări
- Morning Report Obstetri 1Document7 paginiMorning Report Obstetri 1melatiigdÎncă nu există evaluări
- Morning Report Obstetri 12Document5 paginiMorning Report Obstetri 12melatiigdÎncă nu există evaluări
- KPD Drip Oxytocin-18.04.12Document6 paginiKPD Drip Oxytocin-18.04.12Vendi Cahyadi RiandikaÎncă nu există evaluări
- Supervised By: Dr. Punarbawa Spog: Morning ReportDocument19 paginiSupervised By: Dr. Punarbawa Spog: Morning ReportArja' WaasÎncă nu există evaluări
- MR Obgyn LMRDocument25 paginiMR Obgyn LMRRian Segal HidajatÎncă nu există evaluări
- 04-12-13 Letak Sugsang FinishDocument13 pagini04-12-13 Letak Sugsang FinishAnonymous L3q7yHhhÎncă nu există evaluări
- Morning Report: Case Resume Normal Labor 2 Pathology LaborDocument10 paginiMorning Report: Case Resume Normal Labor 2 Pathology LabormelatiigdÎncă nu există evaluări
- Morning Report Obstetri 11Document6 paginiMorning Report Obstetri 11melatiigdÎncă nu există evaluări
- MR PEB Kl1 F Aktif Macet 26.4.12Document6 paginiMR PEB Kl1 F Aktif Macet 26.4.12Arrum Chyntia YuliyantiÎncă nu există evaluări
- Morning Report: Case Resume Normal Labor - Pathology LaborDocument9 paginiMorning Report: Case Resume Normal Labor - Pathology LabormelatiigdÎncă nu există evaluări
- Laporan Kasus PEB + Impending EklamsiaDocument9 paginiLaporan Kasus PEB + Impending EklamsiaPutra MahautamaÎncă nu există evaluări
- Preeklampsia BeratDocument5 paginiPreeklampsia BeratmelatiigdÎncă nu există evaluări
- MR 4 Agustus 2014Document18 paginiMR 4 Agustus 2014Rian Segal HidajatÎncă nu există evaluări
- MR 13Document6 paginiMR 13Vendi Cahyadi RiandikaÎncă nu există evaluări
- Kala II KasepDocument4 paginiKala II KasepSiska SiscaÎncă nu există evaluări
- Supervisor: Dr. Edy Prasetyo, Spog: Medical Student: Novi, Suwika, HeryDocument12 paginiSupervisor: Dr. Edy Prasetyo, Spog: Medical Student: Novi, Suwika, HeryAnonymous L3q7yHhhÎncă nu există evaluări
- Supervisor: Dr. Made Mahayasa, SP - OG Medical Students:: Morning ReportDocument6 paginiSupervisor: Dr. Made Mahayasa, SP - OG Medical Students:: Morning ReportNur LestaryÎncă nu există evaluări
- Morning Report August, 13 2015: Supervisor: Dr. Gede Made Punarbawa, SP - OG DM Jaga: Febri, RianDocument27 paginiMorning Report August, 13 2015: Supervisor: Dr. Gede Made Punarbawa, SP - OG DM Jaga: Febri, RianRian Segal HidajatÎncă nu există evaluări
- DM: Yoga, Ida, Brian, Fauzan, Ardian, Abrista, UlfaDocument21 paginiDM: Yoga, Ida, Brian, Fauzan, Ardian, Abrista, UlfaFaridatun HasanahÎncă nu există evaluări
- Morning Report 1 September 2014Document11 paginiMorning Report 1 September 2014Rian Segal HidajatÎncă nu există evaluări
- MR 29 Sept 2011Document10 paginiMR 29 Sept 2011Lili SurianiÎncă nu există evaluări
- KPD Minggu 9 LalaDocument7 paginiKPD Minggu 9 LalaArja' WaasÎncă nu există evaluări
- Name: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51 Name: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51Document5 paginiName: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51 Name: Mrs. E Age: 26 Yo RM: 538866 Adress: Narmada Admitted: May, 18 2012 at 02.51Akbar GazaliÎncă nu există evaluări
- Morning Report September, 4 2015: Supervisor: Dr. Made Putra Juliawan, Spog DM Jaga: RianDocument48 paginiMorning Report September, 4 2015: Supervisor: Dr. Made Putra Juliawan, Spog DM Jaga: RianRian Segal HidajatÎncă nu există evaluări
- SalmahDocument17 paginiSalmahRian Segal HidajatÎncă nu există evaluări
- Morning Report: Supervised By: Dr. Edi P.W. SpogDocument10 paginiMorning Report: Supervised By: Dr. Edi P.W. SpogArja' WaasÎncă nu există evaluări
- Morning Report VK SCDocument8 paginiMorning Report VK SCmardilasariÎncă nu există evaluări
- Morning Report 16-12-12 Drip SuccessDocument6 paginiMorning Report 16-12-12 Drip SuccessmelatiigdÎncă nu există evaluări
- Preeklampsia BeratDocument9 paginiPreeklampsia BeratmelatiigdÎncă nu există evaluări
- Morning Report 19-12-12 Prolonged Latent PhaseDocument6 paginiMorning Report 19-12-12 Prolonged Latent PhasemelatiigdÎncă nu există evaluări
- Fase Aktif Memanjang Drip & Kala II Lama VEDocument7 paginiFase Aktif Memanjang Drip & Kala II Lama VELaili KhairaniÎncă nu există evaluări
- MR 12 Sept 2011Document7 paginiMR 12 Sept 2011Lili SurianiÎncă nu există evaluări
- 27-10-09 PagiDocument3 pagini27-10-09 PagiLaili KhairaniÎncă nu există evaluări
- Morning Report 31-8-14Document11 paginiMorning Report 31-8-14Rian Segal HidajatÎncă nu există evaluări
- Name: Mrs. S Age: 21 Years Old Address: Penimbun Admitted: January 7 2016 No. RM: 572290Document10 paginiName: Mrs. S Age: 21 Years Old Address: Penimbun Admitted: January 7 2016 No. RM: 572290Meita ReligiaÎncă nu există evaluări
- Supervisor: Dr. Edi Prasetyo W., SP - OG Medical Students:: Morning ReportDocument10 paginiSupervisor: Dr. Edi Prasetyo W., SP - OG Medical Students:: Morning ReportNetii FarhatiÎncă nu există evaluări
- First Stage Active Phase Neglected Pro SCDocument8 paginiFirst Stage Active Phase Neglected Pro SCAYu MiFtakhunÎncă nu există evaluări
- Case Report: IdentityDocument6 paginiCase Report: IdentityKelli RoseÎncă nu există evaluări
- Morning Report October 5 2011: Supervisor: Dr. Doddy, SpogDocument6 paginiMorning Report October 5 2011: Supervisor: Dr. Doddy, SpogLili SurianiÎncă nu există evaluări
- Mr2 KPDP 28 May 2012Document6 paginiMr2 KPDP 28 May 2012Heri Hrisikesa WjgÎncă nu există evaluări
- Duty Report "Example"Document9 paginiDuty Report "Example"Riyan W. PratamaÎncă nu există evaluări
- Supervisor: Dr. Agus Thoriq, Spog DM: AkbarDocument31 paginiSupervisor: Dr. Agus Thoriq, Spog DM: AkbarAkbar GazaliÎncă nu există evaluări
- Morning Report July, 21 2014: Supervisor: Dr. I Made Putra Juliawan, SP - OG DM Jaga: Zia, Yid, Santi, AyuDocument10 paginiMorning Report July, 21 2014: Supervisor: Dr. I Made Putra Juliawan, SP - OG DM Jaga: Zia, Yid, Santi, AyuRian Segal HidajatÎncă nu există evaluări
- MR 25-10-2015 DR - SNO, SP - OG-KDocument57 paginiMR 25-10-2015 DR - SNO, SP - OG-KStephanie Amelia ArgodipuroÎncă nu există evaluări
- 8 NOVEMBER 2009: Morning ReportDocument10 pagini8 NOVEMBER 2009: Morning ReportArja' WaasÎncă nu există evaluări
- 11-10-12 LetliDocument5 pagini11-10-12 LetliArja' WaasÎncă nu există evaluări
- Morning Report 9Document9 paginiMorning Report 9melatiigdÎncă nu există evaluări
- MR Lili Stengah Gemeli Belum JadiDocument5 paginiMR Lili Stengah Gemeli Belum JadiLili SurianiÎncă nu există evaluări
- Morning Report: Supervisor: Dr. H. Doddy Ak., Spog (K)Document10 paginiMorning Report: Supervisor: Dr. H. Doddy Ak., Spog (K)vika handayaniÎncă nu există evaluări
- Morning Report: Case Resume Normal Labor 0 Pathologies LaborDocument5 paginiMorning Report: Case Resume Normal Labor 0 Pathologies LabormelatiigdÎncă nu există evaluări
- HPPDocument15 paginiHPPArizkamhÎncă nu există evaluări
- CPD + MakrosomiaDocument6 paginiCPD + MakrosomiaLili SurianiÎncă nu există evaluări
- DMG + Macrosomnia + APBDocument9 paginiDMG + Macrosomnia + APBArja' WaasÎncă nu există evaluări
- 01 DESEMBER 2008: Morning ReportDocument20 pagini01 DESEMBER 2008: Morning ReportNetii FarhatiÎncă nu există evaluări
- Tumor OvariumDocument20 paginiTumor OvariumPutra MahautamaÎncă nu există evaluări
- Tumor OvariumDocument20 paginiTumor OvariumPutra MahautamaÎncă nu există evaluări
- DistosiaDocument185 paginiDistosiaPutra MahautamaÎncă nu există evaluări
- Physiology of PregnancyDocument31 paginiPhysiology of PregnancyPutra Mahautama100% (1)
- Maternal Physiology During PregnancyDocument28 paginiMaternal Physiology During PregnancyPutra MahautamaÎncă nu există evaluări
- Laporan Kasus KJDRDocument7 paginiLaporan Kasus KJDRPutra MahautamaÎncă nu există evaluări
- Laporan Kasus PEB + Impending EklamsiaDocument9 paginiLaporan Kasus PEB + Impending EklamsiaPutra MahautamaÎncă nu există evaluări
- NCAA Concussion Fact SheetDocument2 paginiNCAA Concussion Fact Sheetelijah edwardsÎncă nu există evaluări
- Angelica Sinensis Materia Medica HerbsDocument3 paginiAngelica Sinensis Materia Medica HerbsAlejandra GuerreroÎncă nu există evaluări
- Research Paper FinalDocument7 paginiResearch Paper Finalapi-643588876Încă nu există evaluări
- Nurse - Resignation LetterDocument1 paginăNurse - Resignation LetterphoenixdashÎncă nu există evaluări
- ORAL REVALIDA (Diabetes Mellitus)Document5 paginiORAL REVALIDA (Diabetes Mellitus)Aubrey Unique EvangelistaÎncă nu există evaluări
- Hsci 360 Long Term Care PPT Revised 9Document23 paginiHsci 360 Long Term Care PPT Revised 9api-249502229Încă nu există evaluări
- Daftar Harga Pengujian Dan Kalibrasi Alat KesehatanDocument3 paginiDaftar Harga Pengujian Dan Kalibrasi Alat KesehatanVIDYA VIRA PAKSYA PUTRAÎncă nu există evaluări
- 198-Article Text-400-2-10-20210427Document8 pagini198-Article Text-400-2-10-20210427rachmatrizqaÎncă nu există evaluări
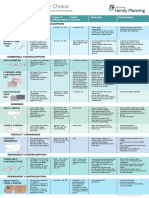
- Contraception Options in New ZealandDocument2 paginiContraception Options in New ZealandStuff NewsroomÎncă nu există evaluări
- Our Noble and Beloved Carroll DunhamDocument2 paginiOur Noble and Beloved Carroll Dunhamkrishna2205Încă nu există evaluări
- Revised OK Sa DepEd Forms 2019 1Document16 paginiRevised OK Sa DepEd Forms 2019 1Marison GerantaÎncă nu există evaluări
- Disaster Nursing NclexDocument5 paginiDisaster Nursing NclexSherrie Mae RoncalÎncă nu există evaluări
- Cerebellar StrokeDocument12 paginiCerebellar StrokewhitecloudsÎncă nu există evaluări
- All-Cause Mortality and Malaria in African Children: Trends and ControversiesDocument32 paginiAll-Cause Mortality and Malaria in African Children: Trends and ControversiesBesong MichaelÎncă nu există evaluări
- To Hospitals & Hospital PhrmacyDocument27 paginiTo Hospitals & Hospital PhrmacyBvayÎncă nu există evaluări
- Nuclear Cardiology: Role in The World of Multimodality Cardiac ImagingDocument5 paginiNuclear Cardiology: Role in The World of Multimodality Cardiac ImagingElena FlorentinaÎncă nu există evaluări
- Benign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramDocument2 paginiBenign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramSimran JosanÎncă nu există evaluări
- Antipsycotic DrugDocument21 paginiAntipsycotic DrugShashank SatheÎncă nu există evaluări
- The African Roots of Traditional Chinese MedicineDocument6 paginiThe African Roots of Traditional Chinese MedicineUniversalLove4LifeÎncă nu există evaluări
- 19-26 Faktor Risiko Kejadian Hipertensi Pada Wanita Usia Subur Di Wilayah Kerja Puskemas NaibonatDocument8 pagini19-26 Faktor Risiko Kejadian Hipertensi Pada Wanita Usia Subur Di Wilayah Kerja Puskemas Naibonatlidya inaÎncă nu există evaluări
- NCM 107 Module 2M Ethico Moral Aspects of NursingDocument18 paginiNCM 107 Module 2M Ethico Moral Aspects of NursingTrisha ApillanesÎncă nu există evaluări
- Martial Arts - Emei Qi Gong-ExercisesDocument3 paginiMartial Arts - Emei Qi Gong-ExercisesSolomon Cosmin Ionut100% (3)
- How To Critically Appraise A PaperDocument6 paginiHow To Critically Appraise A PaperAmbar RahmanÎncă nu există evaluări
- Week 5 Case Study Instructions NR 507Document3 paginiWeek 5 Case Study Instructions NR 507Benedict KakaiÎncă nu există evaluări
- Periodontology 2000 - 2007 - Mombelli - The Diagnosis and Treatment of Peri ImplantitisDocument14 paginiPeriodontology 2000 - 2007 - Mombelli - The Diagnosis and Treatment of Peri Implantitiscinthia210367Încă nu există evaluări
- Reporte 2020 de La Oficina de Asuntos Globales de Estados UnidosDocument72 paginiReporte 2020 de La Oficina de Asuntos Globales de Estados UnidosAristegui NoticiasÎncă nu există evaluări
- Artificial Respiration: ForceDocument15 paginiArtificial Respiration: Forcekushal NeupaneÎncă nu există evaluări
- Angio EdemaDocument172 paginiAngio Edemaalma23roÎncă nu există evaluări
- Pap SmearDocument3 paginiPap SmearcziehjheyÎncă nu există evaluări
- SOP TEC 15 Calculating Drug Doses v1.1Document2 paginiSOP TEC 15 Calculating Drug Doses v1.1rajenderizeÎncă nu există evaluări
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisDe la EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (9)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouDe la EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouÎncă nu există evaluări
- What to Expect When You’re Expecting (5th Edition)De la EverandWhat to Expect When You’re Expecting (5th Edition)Evaluare: 5 din 5 stele5/5 (1)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeDe la EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeÎncă nu există evaluări
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDe la EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeEvaluare: 3.5 din 5 stele3.5/5 (13)
- Pregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!De la EverandPregnancy Hacks: 350+ Easy Hacks for a Happy and Healthy Pregnancy!Evaluare: 5 din 5 stele5/5 (1)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineDe la EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineÎncă nu există evaluări
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicDe la EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicÎncă nu există evaluări
- Reclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeDe la EverandReclaiming Childbirth as a Rite of Passage: Weaving ancient wisdom with modern knowledgeEvaluare: 5 din 5 stele5/5 (16)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenDe la EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenEvaluare: 4 din 5 stele4/5 (154)
- ADHD Women: A Holistic Approach To ADHD ManagementDe la EverandADHD Women: A Holistic Approach To ADHD ManagementEvaluare: 5 din 5 stele5/5 (4)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayDe la EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayEvaluare: 4.5 din 5 stele4.5/5 (3)
- Get the Guy On Your Terms: Proven Dating Advice for Women to Attract Men, Find Love and Build a Relationship that LastsDe la EverandGet the Guy On Your Terms: Proven Dating Advice for Women to Attract Men, Find Love and Build a Relationship that LastsEvaluare: 5 din 5 stele5/5 (18)
- Skinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!De la EverandSkinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!Evaluare: 3.5 din 5 stele3.5/5 (489)
- First Time Dad: The Ultimate Guide for New Dads about Pregnancy Preparation and Childbirth - Advice, Facts, Tips, and Stories for First Time Fathers!De la EverandFirst Time Dad: The Ultimate Guide for New Dads about Pregnancy Preparation and Childbirth - Advice, Facts, Tips, and Stories for First Time Fathers!Evaluare: 5 din 5 stele5/5 (21)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDe la EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisEvaluare: 3 din 5 stele3/5 (2)
- Essential Labor: Mothering as Social ChangeDe la EverandEssential Labor: Mothering as Social ChangeEvaluare: 4 din 5 stele4/5 (25)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.De la EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Evaluare: 4.5 din 5 stele4.5/5 (128)
- Women's Brains: The Female Brain Explained through Neural AnalysesDe la EverandWomen's Brains: The Female Brain Explained through Neural AnalysesEvaluare: 4.5 din 5 stele4.5/5 (22)
- I'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeDe la EverandI'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeEvaluare: 4 din 5 stele4/5 (15)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondDe la EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondEvaluare: 4.5 din 5 stele4.5/5 (3)
- The Strength and Conditioning Bible: How to Train Like an AthleteDe la EverandThe Strength and Conditioning Bible: How to Train Like an AthleteÎncă nu există evaluări
- WomanCode: Perfect Your Cycle, Amplify Your Fertility, Supercharge Your Sex Drive, and Become a Power SourceDe la EverandWomanCode: Perfect Your Cycle, Amplify Your Fertility, Supercharge Your Sex Drive, and Become a Power SourceEvaluare: 4.5 din 5 stele4.5/5 (91)
- The Vegan-Keto Diet Meal Plan: Unexpected Uses for the Ketogenic Diet RecipesDe la EverandThe Vegan-Keto Diet Meal Plan: Unexpected Uses for the Ketogenic Diet RecipesEvaluare: 5 din 5 stele5/5 (1)
- Awakening Fertility: The Essential Art of Preparing for PregnancyDe la EverandAwakening Fertility: The Essential Art of Preparing for PregnancyEvaluare: 4.5 din 5 stele4.5/5 (36)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersDe la EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersEvaluare: 4.5 din 5 stele4.5/5 (72)
- Deaths of Despair and the Future of CapitalismDe la EverandDeaths of Despair and the Future of CapitalismEvaluare: 4.5 din 5 stele4.5/5 (30)
- The Cycle Syncing Handbook: Identify Hormonal Patterns, Build Holistic Habits, and Embrace the Power of Your Menstrual CycleDe la EverandThe Cycle Syncing Handbook: Identify Hormonal Patterns, Build Holistic Habits, and Embrace the Power of Your Menstrual CycleÎncă nu există evaluări