S-ar putea să vă placă și
- NCPDocument2 paginiNCPDidith AbanÎncă nu există evaluări
- NCP Rheumatic Heart DiseaseDocument3 paginiNCP Rheumatic Heart DiseaseAdrian Mallar71% (28)
- NCP (Rheumatic Heart Disease)Document2 paginiNCP (Rheumatic Heart Disease)Jenny Ajoc75% (4)
- NURSING CARE PLAN Decreased Cardiac Output FnaDocument2 paginiNURSING CARE PLAN Decreased Cardiac Output FnaAce Dioso Tubasco100% (1)
- Myocarditis NCP 2Document8 paginiMyocarditis NCP 2astro_aaron117375% (4)
- NCP Near DrowningDocument1 paginăNCP Near Drowningchristine louise bernardoÎncă nu există evaluări
- Ineffective Airway Clearance Related To BronchospasmDocument2 paginiIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- NCPDocument4 paginiNCPEsther RefuncionÎncă nu există evaluări
- Nursing Care PlanDocument7 paginiNursing Care PlanGem Ma100% (7)
- NCP For Mi PainDocument2 paginiNCP For Mi PainKahMallariÎncă nu există evaluări
- Risk For Decreased Cardiac OutputDocument3 paginiRisk For Decreased Cardiac OutputSid Artemis FriasÎncă nu există evaluări
- Nursing Care PlanDocument4 paginiNursing Care PlanJoshua Pascasio100% (1)
- SAMPLE NCP For Pernicious AnemiaDocument3 paginiSAMPLE NCP For Pernicious Anemiainks19100% (7)
- Nursing Interventions for Ineffective Breathing PatternDocument1 paginăNursing Interventions for Ineffective Breathing PatternnikkilyceeÎncă nu există evaluări
- Disturbed Visual Sensory Perception Related: Nursing Care PlanDocument3 paginiDisturbed Visual Sensory Perception Related: Nursing Care PlanMae Therese B. MAGNOÎncă nu există evaluări
- NCP Activity IntoleranceDocument5 paginiNCP Activity IntoleranceRea HashimÎncă nu există evaluări
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Nursing Care PlansDocument21 pagini"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Nursing Care PlansCarl Elexer Cuyugan Ano100% (1)
- Rheumatic Heart Disease - CSDocument88 paginiRheumatic Heart Disease - CSMASII100% (7)
- Promoting Optimal Sleep Patterns Through Non-Pharmacological InterventionsDocument2 paginiPromoting Optimal Sleep Patterns Through Non-Pharmacological InterventionsNoriel LacsinaÎncă nu există evaluări
- Acute Coronary Syndrome NCP 03Document6 paginiAcute Coronary Syndrome NCP 03AgronaSlaughterÎncă nu există evaluări
- NCP PneumothoraxDocument3 paginiNCP Pneumothorax'Harold Mark Borja100% (2)
- Cardiovascular Disease NCPDocument5 paginiCardiovascular Disease NCPShyla ManguiatÎncă nu există evaluări
- Nursing Care Plan For A Patient With Pleural EffusionDocument5 paginiNursing Care Plan For A Patient With Pleural Effusionmac042250% (4)
- NURSING-CARE-PLAN-Lung-Cancerxxx 1Document3 paginiNURSING-CARE-PLAN-Lung-Cancerxxx 1Caroline ChaÎncă nu există evaluări
- NCPDocument4 paginiNCPElbert Vierneza100% (2)
- NCP for Acute Coronary Syndrome AssessmentDocument3 paginiNCP for Acute Coronary Syndrome Assessmentsarahtot67% (3)
- Assessing Ascites in a Patient with Liver DiseaseDocument1 paginăAssessing Ascites in a Patient with Liver Diseasehaniehaehae100% (1)
- NCP For Pleural EffusionDocument4 paginiNCP For Pleural EffusionLilian Linogao71% (7)
- NCPDocument3 paginiNCPChrisTine M. MoralesÎncă nu există evaluări
- Activity IntoleranceDocument3 paginiActivity IntoleranceGen RodriguezÎncă nu există evaluări
- RHD Case StudyDocument94 paginiRHD Case StudyGel Jovenal100% (1)
- Decreased Cardiac OutputDocument4 paginiDecreased Cardiac OutputChristine MatasÎncă nu există evaluări
- 17Y Patient Pleural Effusion CareDocument4 pagini17Y Patient Pleural Effusion CareTrixie Anne GamotinÎncă nu există evaluări
- Care Plan Prep May 13 Rheumatic FeverDocument16 paginiCare Plan Prep May 13 Rheumatic Feverapi-256360167Încă nu există evaluări
- Risk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Document2 paginiRisk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Yessamin Paith Roderos100% (1)
- NCP - EdemaDocument1 paginăNCP - Edemavipncpusers100% (1)
- Care Plan ExampleDocument2 paginiCare Plan Exampleincess27100% (1)
- NCP Increased IcpDocument2 paginiNCP Increased IcphelloaÎncă nu există evaluări
- Multiple MyelomaDocument2 paginiMultiple MyelomaKolin JandocÎncă nu există evaluări
- NCP (Icu)Document2 paginiNCP (Icu)jessie_nuñez_263% (8)
- Nursing Care Plan for Post-Op PatientDocument3 paginiNursing Care Plan for Post-Op Patientromelyn100% (1)
- Headache Nursing CareDocument4 paginiHeadache Nursing CareAnneUXDÎncă nu există evaluări
- Adhf NCPDocument3 paginiAdhf NCPkristine keen buanÎncă nu există evaluări
- Coronary Artery Disease Care PlanDocument2 paginiCoronary Artery Disease Care PlanDanelle Harrison, RN100% (2)
- Decreased Cardiac OutputDocument3 paginiDecreased Cardiac OutputTiffany Mathis100% (1)
- NCP Heart FailureDocument2 paginiNCP Heart FailureDayan Cabriga100% (1)
- Compromised Family Coping NCPDocument2 paginiCompromised Family Coping NCPJamaeka Gotis100% (1)
- Ineffective Breathing Pattern Related To Bronchospasm, Decreased Lung ExpansionDocument2 paginiIneffective Breathing Pattern Related To Bronchospasm, Decreased Lung ExpansionReylan Garcia43% (7)
- Nursing Care Plan 1 DiagDocument4 paginiNursing Care Plan 1 Diagguysornngam100% (1)
- NCP - Ineffective Airway ClearanceDocument2 paginiNCP - Ineffective Airway ClearanceKhat100% (1)
- ANDAYA, Kristine Alexis L. BSN218 Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 paginiANDAYA, Kristine Alexis L. BSN218 Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale EvaluationAlexis TineÎncă nu există evaluări
- Nursing Care Plan for GastroenteritisDocument7 paginiNursing Care Plan for GastroenteritisChris Denver BancaleÎncă nu există evaluări
- Acute Coronary Syndrome NCP 02Document6 paginiAcute Coronary Syndrome NCP 02AgronaSlaughterÎncă nu există evaluări
- NCP Inffective Tissue PerfusionDocument3 paginiNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- NCPDocument9 paginiNCPTracy Camille EscobarÎncă nu există evaluări
- NCP For CHFDocument2 paginiNCP For CHFMayet De Castro Lejano100% (1)
- Ineffective Tissue Perfusion Related To Decrease Hemoglobin Concentration in The BloodDocument2 paginiIneffective Tissue Perfusion Related To Decrease Hemoglobin Concentration in The BloodYllejann Manez60% (20)
- NCP-Case Presentation (CHF)Document4 paginiNCP-Case Presentation (CHF)Jessamine EnriquezÎncă nu există evaluări
- NCP For EclampsiaDocument6 paginiNCP For EclampsiaXtine Soliman Zamora100% (3)
- RetinalDocument11 paginiRetinalHenry Roque TagalagÎncă nu există evaluări
- RiskDocument1 paginăRiskHenry Roque TagalagÎncă nu există evaluări
- Case Study On Ob Ward PreeclampsiaDocument12 paginiCase Study On Ob Ward PreeclampsiaNimrod83% (6)
- Wesleyan University - Philippines: Delivery Cases (Assist)Document6 paginiWesleyan University - Philippines: Delivery Cases (Assist)Henry Roque TagalagÎncă nu există evaluări
- Thesis Study Habits Ms WordDocument2 paginiThesis Study Habits Ms WordHenry Roque TagalagÎncă nu există evaluări
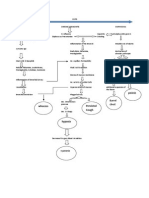
- Copd PathoDocument1 paginăCopd PathoHenry Roque TagalagÎncă nu există evaluări
- Diseases Affecting Mhjkkthe Circulatory SystemDocument4 paginiDiseases Affecting Mhjkkthe Circulatory SystemHenry Roque TagalagÎncă nu există evaluări
- Act NorhrhhDocument1 paginăAct NorhrhhHenry Roque TagalagÎncă nu există evaluări
- Undifferentiated SchizophreniaDocument190 paginiUndifferentiated Schizophreniaallexiscampaner100% (16)
- Checklist-Ncm 104 (Skills) (2hjjhjDocument10 paginiChecklist-Ncm 104 (Skills) (2hjjhjHenry Roque TagalagÎncă nu există evaluări
- Act NorhrhhDocument1 paginăAct NorhrhhHenry Roque TagalagÎncă nu există evaluări
- Drug StudyDocument40 paginiDrug Studyapi-374468390% (61)
- Case Study RheumaticDocument46 paginiCase Study RheumaticJill Anne Balderosa91% (11)
- Tracheostomy Skin Care (Stoma Care)Document4 paginiTracheostomy Skin Care (Stoma Care)Henry Roque TagalagÎncă nu există evaluări
- MultivitaminDocument1 paginăMultivitaminKatie McPeek88% (8)
- Azithromycin (Drug Study)Document2 paginiAzithromycin (Drug Study)Franz.thenurse688893% (15)
- Dada Choose My PlateDocument1 paginăDada Choose My PlateHenry Roque TagalagÎncă nu există evaluări
- Pathophysiology BPH Case StudyDocument3 paginiPathophysiology BPH Case Studyyhanne100% (24)
- FluimucilDocument2 paginiFluimucilianecunar86% (7)
- FluimucilDocument2 paginiFluimucilianecunar86% (7)
- Risk Factors in AtherosclerosisDocument1 paginăRisk Factors in AtherosclerosisHenry Roque TagalagÎncă nu există evaluări
- Pathophysiology BPH Case StudyDocument3 paginiPathophysiology BPH Case Studyyhanne100% (24)
- DB13 - Pathophysiology of AtherosclerosisDocument2 paginiDB13 - Pathophysiology of Atherosclerosisi_vhie03Încă nu există evaluări
- A Nursing Care Plan VaDocument3 paginiA Nursing Care Plan VaArianne Paola QuindoyÎncă nu există evaluări
- Drug Study AminophyllineDocument1 paginăDrug Study Aminophyllinejunie100% (3)
- Nursing Minimum Data Set SystemDocument4 paginiNursing Minimum Data Set SystemHenry Roque Tagalag100% (3)
- Drug Study AminophyllineDocument1 paginăDrug Study Aminophyllinejunie100% (3)
- Drug Study AminophyllineDocument1 paginăDrug Study Aminophyllinejunie100% (3)
- NCP of CavDocument3 paginiNCP of CavHenry Roque TagalagÎncă nu există evaluări
- CHAPTER 3 Non-Communicable Disease EpidemiologyDocument24 paginiCHAPTER 3 Non-Communicable Disease EpidemiologyteklayÎncă nu există evaluări
- "Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewDocument6 pagini"Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Renee IOWL - Workbook - 1 - 18Document182 paginiRenee IOWL - Workbook - 1 - 18Mirna Velazquez100% (1)
- Ilovepdf MergedDocument351 paginiIlovepdf MergedSwara SawantÎncă nu există evaluări
- Screening For Microalbuminuria in Patients With Diabetes: How? Why?Document2 paginiScreening For Microalbuminuria in Patients With Diabetes: How? Why?Abhishek SenÎncă nu există evaluări
- Baiae NCPDocument1 paginăBaiae NCPreignyfayeÎncă nu există evaluări
- Remember This - FoerDocument2 paginiRemember This - FoerElham AhmedÎncă nu există evaluări
- Diabetes: World Journal ofDocument14 paginiDiabetes: World Journal ofdesytrilistyoatiÎncă nu există evaluări
- The Role of Epidemiology in Public HealthDocument19 paginiThe Role of Epidemiology in Public HealthGilbert LimenÎncă nu există evaluări
- Nursing Assessment and Interventions for Episiotomy Wound CareDocument2 paginiNursing Assessment and Interventions for Episiotomy Wound Carenethcecilia90% (10)
- Top 8 Pain Herbs EbookDocument35 paginiTop 8 Pain Herbs EbookMari BuôgoÎncă nu există evaluări
- Social Anxiety Disorder 1.editedDocument4 paginiSocial Anxiety Disorder 1.editedmoureenÎncă nu există evaluări
- East Meets West From The Bottom Up - Chapter 11 "Phantom & Opera"Document5 paginiEast Meets West From The Bottom Up - Chapter 11 "Phantom & Opera"nyhartp2457Încă nu există evaluări
- The DNA Way - Kashif KhanDocument268 paginiThe DNA Way - Kashif Khancepa100% (1)
- Powerpoint: Colorectal Surgical DiseasesDocument74 paginiPowerpoint: Colorectal Surgical Diseasesj.doe.hex_87100% (1)
- Balance Retraining YardleyDocument10 paginiBalance Retraining YardleystepwiseclicheÎncă nu există evaluări
- Development of Cinnamon Oil Based Topical Formulations for their Antibacterial ActivityDocument17 paginiDevelopment of Cinnamon Oil Based Topical Formulations for their Antibacterial ActivityKristen TeeÎncă nu există evaluări
- Artritis Gout in Aviation MedicineDocument22 paginiArtritis Gout in Aviation MedicineBuyungÎncă nu există evaluări
- Journal ReadingDocument17 paginiJournal ReadingDesty Friska KurniaÎncă nu există evaluări
- Delmar's Pediatric Nursing Care Plans, 3 Edition, Karla L. Luxner, RNC, ND, Pg. 67Document2 paginiDelmar's Pediatric Nursing Care Plans, 3 Edition, Karla L. Luxner, RNC, ND, Pg. 67KMÎncă nu există evaluări
- Cuz End of Term 3 MCQ Surgery1 Sept 2020Document14 paginiCuz End of Term 3 MCQ Surgery1 Sept 2020MustafaÎncă nu există evaluări
- Understanding Dilated Cardiomyopathy: Signs, Symptoms, Nursing CareDocument93 paginiUnderstanding Dilated Cardiomyopathy: Signs, Symptoms, Nursing CareE.J. PelayoÎncă nu există evaluări
- Presenting Compliants: Centra Nervous SystemDocument6 paginiPresenting Compliants: Centra Nervous SystemMOWNIANÎncă nu există evaluări
- Assignment 4 MHPPDocument11 paginiAssignment 4 MHPPBabar AliÎncă nu există evaluări
- The "when" and "where" of α-synucleinopathies: Insights from REM sleep behavior disorderDocument3 paginiThe "when" and "where" of α-synucleinopathies: Insights from REM sleep behavior disorderSandsackÎncă nu există evaluări
- Personality DisordersDocument5 paginiPersonality Disordersapi-274059472Încă nu există evaluări
- Lepra 2022Document4 paginiLepra 2022Ketut ArtawanÎncă nu există evaluări
- Family CoDocument52 paginiFamily ComansiagrawalÎncă nu există evaluări
- Rasa Guna Vierya & Probhava: Understanding Ayurvedic Tastes, Qualities, Potency and Special EffectsDocument7 paginiRasa Guna Vierya & Probhava: Understanding Ayurvedic Tastes, Qualities, Potency and Special EffectsSN WijesinheÎncă nu există evaluări
- List Nama Cantik & Kel. Yel-Yel 2022Document3 paginiList Nama Cantik & Kel. Yel-Yel 2022Daffa RamadhaniÎncă nu există evaluări