S-ar putea să vă placă și
- PhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueDocument14 paginiPhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueChrysanthus HerreraÎncă nu există evaluări
- Ra 10354Document13 paginiRa 10354CBCP for LifeÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesDocument22 paginiPhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesChrysanthus Herrera100% (2)
- PhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesDocument98 paginiPhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesChrysanthus Herrera50% (2)
- CF1Document1 paginăCF1Kim ViñasÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesDocument111 paginiPhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesChrysanthus Herrera80% (5)
- PhilHealth Circular No. 0035, s.2013 Annex 4 Examples and Scenarios For The All Case Rates Implementing GuidelinesDocument7 paginiPhilHealth Circular No. 0035, s.2013 Annex 4 Examples and Scenarios For The All Case Rates Implementing GuidelinesChrysanthus HerreraÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityDocument11 paginiPhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityChrysanthus HerreraÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex11 PhilHealthClaimForm3 Frontpage (RevisedNovember2013)Document2 paginiPhilHealth Circular No. 0035, s.2013 Annex11 PhilHealthClaimForm3 Frontpage (RevisedNovember2013)Chrysanthus HerreraÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex 3 List of Medical Conditions and Procedures Allowed As Second Case RateDocument31 paginiPhilHealth Circular No. 0035, s.2013 Annex 3 List of Medical Conditions and Procedures Allowed As Second Case RateChrysanthus Herrera0% (1)
- PhilHealth Circular No. 0035, s.2013 Annex 8 List of Medical Conditions Allowed For Referral PackageDocument7 paginiPhilHealth Circular No. 0035, s.2013 Annex 8 List of Medical Conditions Allowed For Referral PackageChrysanthus HerreraÎncă nu există evaluări
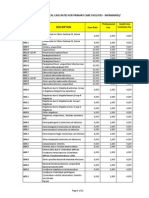
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 paginiPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraÎncă nu există evaluări
- PhilHealth ClaimForm1 GuidelinesDocument4 paginiPhilHealth ClaimForm1 GuidelinesAsh CampiaoÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex 9 Referral FormDocument1 paginăPhilHealth Circular No. 0035, s.2013 Annex 9 Referral FormChrysanthus HerreraÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Document2 paginiPhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Chrysanthus HerreraÎncă nu există evaluări
- PhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Document8 paginiPhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Chrysanthus HerreraÎncă nu există evaluări
- Annex11 ImportantRemindersForThePhilHealthClaimForms (November2013)Document2 paginiAnnex11 ImportantRemindersForThePhilHealthClaimForms (November2013)Chrysanthus HerreraÎncă nu există evaluări
- Philippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesDocument17 paginiPhilippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesChrysanthus HerreraÎncă nu există evaluări
- Tabata WorkoutDocument1 paginăTabata WorkoutEmily HeadingsÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)