S-ar putea să vă placă și
- Problem-based Approach to Gastroenterology and HepatologyDe la EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisÎncă nu există evaluări
- ACOG Practice Bulletin No137 PDFDocument11 paginiACOG Practice Bulletin No137 PDFRodrigo Pérez CuelloÎncă nu există evaluări
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionDe la EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionÎncă nu există evaluări
- Transverse Cerebellar Measurement Fetal AgeDocument96 paginiTransverse Cerebellar Measurement Fetal Ageparas yadav100% (1)
- Ion Channels in Health and DiseaseDe la EverandIon Channels in Health and DiseaseGeoffrey S. PittÎncă nu există evaluări
- Acog SDR AntifosfolipidicDocument8 paginiAcog SDR Antifosfolipidicleonar8Încă nu există evaluări
- Acog 19Document25 paginiAcog 19Janet GoldameirÎncă nu există evaluări
- 2023 OB/GYN Coding Manual: Components of Correct CodingDe la Everand2023 OB/GYN Coding Manual: Components of Correct CodingÎncă nu există evaluări
- Nausea and Vomiting of Pregnancy and Hyperemesis GravidarumDocument27 paginiNausea and Vomiting of Pregnancy and Hyperemesis GravidarumxxdrivexxÎncă nu există evaluări
- ACOG Practice Bulletin No. 202 - Hipertensión Gestacional y ... - Obstetricia y Ginecología PDFDocument36 paginiACOG Practice Bulletin No. 202 - Hipertensión Gestacional y ... - Obstetricia y Ginecología PDFAnghelino Jesus Meza CentenoÎncă nu există evaluări
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2De la EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2Încă nu există evaluări
- Dengue Fever and Pregnancy-A Review and CommentDocument6 paginiDengue Fever and Pregnancy-A Review and CommentRolando AgustianÎncă nu există evaluări
- Dystocia and Augmentation of LAbor PDFDocument10 paginiDystocia and Augmentation of LAbor PDFKathleenÎncă nu există evaluări
- Preterm Prelabour Rupture of MembranesDocument12 paginiPreterm Prelabour Rupture of MembranesSeptiany Indahsari DjanÎncă nu există evaluări
- ACOG Tech BullitinDocument20 paginiACOG Tech BullitinJosephÎncă nu există evaluări
- Practice Bulletin: Antiphospholipid SyndromeDocument8 paginiPractice Bulletin: Antiphospholipid SyndromeSus ArÎncă nu există evaluări
- 002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFDocument11 pagini002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFale_fearÎncă nu există evaluări
- Gyne LE 2: Stage IVA Is Characterized byDocument49 paginiGyne LE 2: Stage IVA Is Characterized byĐinesh IlavarasanÎncă nu există evaluări
- CPG DyslipidemiaDocument26 paginiCPG DyslipidemiaRenzy SalumbreÎncă nu există evaluări
- Uterine Artery Malformation1Document9 paginiUterine Artery Malformation1venkayammaÎncă nu există evaluări
- Leiomioma - TratamientoDocument37 paginiLeiomioma - TratamientoNella SolanoÎncă nu există evaluări
- Gestational Trophoblastic DiseaseDocument6 paginiGestational Trophoblastic DiseaseSJ IraaÎncă nu există evaluări
- Premature Rupture of Membranes 2016Document13 paginiPremature Rupture of Membranes 2016Berenice TrejoÎncă nu există evaluări
- Pre-And Post-Book Study Test For The Shelf Exam: How To Use This ChapterDocument6 paginiPre-And Post-Book Study Test For The Shelf Exam: How To Use This ChapterMiguel CuevasÎncă nu există evaluări
- Oral Boards 2Document67 paginiOral Boards 2Steven GodelmanÎncă nu există evaluări
- 1.10 CPG For TBDocument9 pagini1.10 CPG For TBMaikka IlaganÎncă nu există evaluări
- Poly Hi DR AmnionDocument7 paginiPoly Hi DR Amnionwanwan_adongÎncă nu există evaluări
- Postpartum CollapseDocument54 paginiPostpartum Collapsemedical chroniclesÎncă nu există evaluări
- Hipercalcemia JamaDocument13 paginiHipercalcemia JamaSebastián Camilo Duque100% (1)
- Management of CA Vulva 2Document33 paginiManagement of CA Vulva 2api-3705046Încă nu există evaluări
- Acute Kidney InjuryDocument15 paginiAcute Kidney InjuryManish VijayÎncă nu există evaluări
- Obstetric Highlights Elmar P. Sakala PDFDocument47 paginiObstetric Highlights Elmar P. Sakala PDFwalt65Încă nu există evaluări
- App 2021 AcogDocument26 paginiApp 2021 AcogFernanda Copete Yolianis100% (1)
- Acog 194Document15 paginiAcog 194Marco DiestraÎncă nu există evaluări
- Diabetes Pregestacional ACOGDocument21 paginiDiabetes Pregestacional ACOGarturoÎncă nu există evaluări
- Acog - Practice Bulletin Gynecology PDFDocument486 paginiAcog - Practice Bulletin Gynecology PDFali alrashediÎncă nu există evaluări
- Pocketbookofobstetricneonatalnpediatricemergencies PDFDocument378 paginiPocketbookofobstetricneonatalnpediatricemergencies PDFDANAÎncă nu există evaluări
- Maternal Collapse During PregnancyDocument57 paginiMaternal Collapse During PregnancytapayanaÎncă nu există evaluări
- ACOG Bulletin MiscarriageDocument12 paginiACOG Bulletin Miscarriagebrabba19856403Încă nu există evaluări
- Pancreatic CancerDocument4 paginiPancreatic Cancersdf100% (1)
- Ectopic PregnancyDocument24 paginiEctopic PregnancybertouwÎncă nu există evaluări
- Ultrasound Fundamentals An Evidence Based Guide For Medical PractitionersDocument372 paginiUltrasound Fundamentals An Evidence Based Guide For Medical Practitionersahmet kutluayÎncă nu există evaluări
- ResucNeonatBasica OMSDocument65 paginiResucNeonatBasica OMSAsPonceMichÎncă nu există evaluări
- Diabetes Acog 2017Document15 paginiDiabetes Acog 2017Holger Vicente Guerrero Guerrero100% (1)
- Diagnosis & Management of Preeclampsia & Eclampsia PDFDocument9 paginiDiagnosis & Management of Preeclampsia & Eclampsia PDFBerri RahmadhoniÎncă nu există evaluări
- 3 Medical HistoryDocument101 pagini3 Medical HistoryHamsawiÎncă nu există evaluări
- Acute Pancreatitis: in The ClinicDocument16 paginiAcute Pancreatitis: in The ClinicdeltanueveÎncă nu există evaluări
- AUB Classification - FIGODocument8 paginiAUB Classification - FIGOjeansabalosÎncă nu există evaluări
- Hemorragia Posparto-AcogDocument19 paginiHemorragia Posparto-AcogCristian LaraÎncă nu există evaluări
- Fetal ArrhythmiasDocument18 paginiFetal ArrhythmiasKarin Stefanny Muñoz CastilloÎncă nu există evaluări
- DIT 2013 WorksheetDocument524 paginiDIT 2013 Worksheetsza5031100% (3)
- ACOG Practice Bulletin On Thyroid Disease in PregnancyDocument5 paginiACOG Practice Bulletin On Thyroid Disease in Pregnancygenerics54321Încă nu există evaluări
- ACOG 2009 Induction of LaborDocument12 paginiACOG 2009 Induction of LaborRiantiara PutrizaÎncă nu există evaluări
- Revision Long Case Obs GynaeDocument10 paginiRevision Long Case Obs GynaeHo Yong WaiÎncă nu există evaluări
- Ultrasound in 1st, 2nd & 3rd trimester د.رامز الأسوديDocument13 paginiUltrasound in 1st, 2nd & 3rd trimester د.رامز الأسوديMohammad BelbahaithÎncă nu există evaluări
- OBSTETRICS AND GYNAECOLOGY CollectionDocument12 paginiOBSTETRICS AND GYNAECOLOGY CollectionAhmad Syahmi YZÎncă nu există evaluări
- Section A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Document13 paginiSection A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Sheldon FerronÎncă nu există evaluări
- Obgm Feb2018 Vol.30 No.2 PDFDocument55 paginiObgm Feb2018 Vol.30 No.2 PDFlcmurilloÎncă nu există evaluări
- Pregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervalDocument3 paginiPregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervallcmurilloÎncă nu există evaluări
- Patient-Centered Risk Assessment For Ovarian CancerDocument13 paginiPatient-Centered Risk Assessment For Ovarian CancerlcmurilloÎncă nu există evaluări
- Alteration of The Hormone-Free IntervalDocument2 paginiAlteration of The Hormone-Free IntervalAnonymous d4X4wZLDÎncă nu există evaluări
- Obgm Mar2018 Vol.30 No.3Document57 paginiObgm Mar2018 Vol.30 No.3lcmurilloÎncă nu există evaluări
- ACOG Practice Advisory On Annual Pelvic Examination RecommendationsDocument1 paginăACOG Practice Advisory On Annual Pelvic Examination RecommendationslcmurilloÎncă nu există evaluări
- Tamizaje CancerDocument1 paginăTamizaje CancerlcmurilloÎncă nu există evaluări
- Obgm Modern Day Laboring FinalDocument8 paginiObgm Modern Day Laboring FinallcmurilloÎncă nu există evaluări
- Obgm Mar2018 Vol.30 No.3Document57 paginiObgm Mar2018 Vol.30 No.3lcmurilloÎncă nu există evaluări
- Caffeine Intake - Even Dad's - Linked To Miscarriage, Study Says - MedlinePlusDocument3 paginiCaffeine Intake - Even Dad's - Linked To Miscarriage, Study Says - MedlinePluslcmurilloÎncă nu există evaluări
- A Randomized Trial Comparing SkinDocument9 paginiA Randomized Trial Comparing SkinlcmurilloÎncă nu există evaluări
- P 4065Document2 paginiP 4065lcmurilloÎncă nu există evaluări
- Everyday Contraception ConsiderationsDocument15 paginiEveryday Contraception ConsiderationslcmurilloÎncă nu există evaluări
- 11complications of Unsafe Abortion in Sub-SaharanDocument15 pagini11complications of Unsafe Abortion in Sub-SaharanlcmurilloÎncă nu există evaluări
- Pelvic Examination 3Document1 paginăPelvic Examination 3lcmurilloÎncă nu există evaluări
- Pelvic ExaminationDocument14 paginiPelvic ExaminationlcmurilloÎncă nu există evaluări
- HBV Screening 4Document1 paginăHBV Screening 4lcmurilloÎncă nu există evaluări
- HBV Screening 5Document3 paginiHBV Screening 5lcmurilloÎncă nu există evaluări
- HBV ScreeningDocument24 paginiHBV ScreeninglcmurilloÎncă nu există evaluări
- Pi Is 074937970300120 XDocument7 paginiPi Is 074937970300120 XlcmurilloÎncă nu există evaluări
- 2013 Recommended Adolescent ImmunizationDocument2 pagini2013 Recommended Adolescent ImmunizationArvi MandaweÎncă nu există evaluări
- Parent Ver SCH 0 6yrsDocument2 paginiParent Ver SCH 0 6yrslcmurilloÎncă nu există evaluări
- Pelvic Examination 2Document7 paginiPelvic Examination 2lcmurilloÎncă nu există evaluări
- HBV Screening 2Document10 paginiHBV Screening 2lcmurilloÎncă nu există evaluări
- P 4036Document3 paginiP 4036lcmurilloÎncă nu există evaluări
- P 4060Document2 paginiP 4060lcmurilloÎncă nu există evaluări
- Catchup ScheduleDocument4 paginiCatchup ScheduleAisha SyedÎncă nu există evaluări
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 paginiSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)gyna_2002Încă nu există evaluări
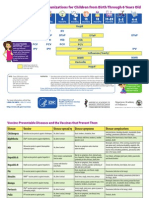
- 04 Immunizations and Developmental Milestones For Your Child From Birth Through 6 Years OldDocument2 pagini04 Immunizations and Developmental Milestones For Your Child From Birth Through 6 Years Oldapi-309082881Încă nu există evaluări
- Foundation of Nursing Practice Exam For Infection Asepsis Basic Concept of Stress and IllnessDocument34 paginiFoundation of Nursing Practice Exam For Infection Asepsis Basic Concept of Stress and IllnessAdrian MiguelÎncă nu există evaluări
- Community Dentistry ReviewerDocument2 paginiCommunity Dentistry ReviewerCzarina DavidÎncă nu există evaluări
- Argumentative Essay Plastic SurgeryDocument3 paginiArgumentative Essay Plastic SurgeryCatherine BaniquedÎncă nu există evaluări
- Predictors of Patient Satisfaction: Jeffrey L. Jackson, Judith Chamberlin, Kurt KroenkeDocument12 paginiPredictors of Patient Satisfaction: Jeffrey L. Jackson, Judith Chamberlin, Kurt Kroenkealina petreÎncă nu există evaluări
- Tubulointerstitial Nephritis, 2022Document344 paginiTubulointerstitial Nephritis, 2022Fercho MedÎncă nu există evaluări
- English For The Professional NurseDocument12 paginiEnglish For The Professional NurseOryza SativaÎncă nu există evaluări
- AcuDose-Rx Users Experience Improved Patient Care, Reduced Pharmacy Turnaround Times, TighterMedication SecurityDocument2 paginiAcuDose-Rx Users Experience Improved Patient Care, Reduced Pharmacy Turnaround Times, TighterMedication SecurityAcudoserxÎncă nu există evaluări
- Details of Students Admitted Through NEET PG 2020-21-701 1400Document700 paginiDetails of Students Admitted Through NEET PG 2020-21-701 1400Minerva Medical Treatment Pvt LtdÎncă nu există evaluări
- Pharmaceutical Sciences: The Covid-19 Pandemic and Its Impact On Human BeingsDocument3 paginiPharmaceutical Sciences: The Covid-19 Pandemic and Its Impact On Human BeingsiajpsÎncă nu există evaluări
- Case Study - Anxiety and Anxiety DisordersDocument2 paginiCase Study - Anxiety and Anxiety DisordersCamille SindayÎncă nu există evaluări
- OSCE Checklist Obstetric History TakingDocument3 paginiOSCE Checklist Obstetric History TakingAhmed Abdel-naserÎncă nu există evaluări
- A Case Study On Employee Engagement: Marriott International, IncDocument12 paginiA Case Study On Employee Engagement: Marriott International, IncPreeti Singh Yadav Student, Jaipuria LucknowÎncă nu există evaluări
- Cecil C. Steiner (X396 - 1: Dentqfnc OnhopDocument2 paginiCecil C. Steiner (X396 - 1: Dentqfnc OnhopClaudia Gamboa Ferrer100% (2)
- Effects of Knowledge Management On Competitive AdvantageDocument67 paginiEffects of Knowledge Management On Competitive AdvantageBenard Webuye100% (1)
- Healthsmart Design Authority: Ihi Pre-Implementation ProjectDocument31 paginiHealthsmart Design Authority: Ihi Pre-Implementation Projectwidayat81Încă nu există evaluări
- Bleeding After Tooth ExtractionDocument3 paginiBleeding After Tooth ExtractionwahyurianjaniÎncă nu există evaluări
- Alexis Mirar PcsoDocument3 paginiAlexis Mirar Pcsodivine mercyÎncă nu există evaluări
- Ashley M Hannah - Resume 2017Document2 paginiAshley M Hannah - Resume 2017api-358481330Încă nu există evaluări
- Kidney TransplantationDocument780 paginiKidney TransplantationJessica ArciniegasÎncă nu există evaluări
- Prof. Herkutanto - Informed Consent Sebagai Pencegahan Tuntutan 2017Document33 paginiProf. Herkutanto - Informed Consent Sebagai Pencegahan Tuntutan 2017muslih setia ardi cahyanaÎncă nu există evaluări
- Diagnostic 20231124083541Document1 paginăDiagnostic 20231124083541Lucia LizardaÎncă nu există evaluări
- Ellex Glaucoma BrochureDocument12 paginiEllex Glaucoma BrochureHaag-Streit UK (HS-UK)Încă nu există evaluări
- Overview of Mental Health and Psychosocial SupportDocument13 paginiOverview of Mental Health and Psychosocial Supportselin uyÎncă nu există evaluări
- Crystal Medici Resume 2021Document3 paginiCrystal Medici Resume 2021api-556030981Încă nu există evaluări
- Final Paper, Substance Abuse in The ElderlyDocument15 paginiFinal Paper, Substance Abuse in The ElderlyalexiscurranÎncă nu există evaluări
- General Competency Radiology In-Training Test Questions For Diagnostic Radiology ResidentsDocument9 paginiGeneral Competency Radiology In-Training Test Questions For Diagnostic Radiology ResidentsSabinaÎncă nu există evaluări
- 2020 Global Health Care Outlook: Laying A Foundation For The FutureDocument1 pagină2020 Global Health Care Outlook: Laying A Foundation For The FutureAlvaro SánchezÎncă nu există evaluări
- Garrenton Nursing Skills Checklist 2022Document7 paginiGarrenton Nursing Skills Checklist 2022api-507789841Încă nu există evaluări
- Pediatric Transplant Rating InstrumentDocument10 paginiPediatric Transplant Rating InstrumentcoxalfonsoÎncă nu există evaluări
- Health Disparity and Literacy PaperDocument5 paginiHealth Disparity and Literacy PaperlameckwesiÎncă nu există evaluări
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodDe la EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodEvaluare: 5 din 5 stele5/5 (33)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDe la EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisEvaluare: 3 din 5 stele3/5 (2)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayDe la EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayEvaluare: 5 din 5 stele5/5 (2)
- What to Expect When You’re Expecting (5th Edition)De la EverandWhat to Expect When You’re Expecting (5th Edition)Evaluare: 5 din 5 stele5/5 (1)
- ADHD Women: A Holistic Approach To ADHD ManagementDe la EverandADHD Women: A Holistic Approach To ADHD ManagementEvaluare: 5 din 5 stele5/5 (4)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDe la EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeEvaluare: 3.5 din 5 stele3.5/5 (13)
- Awakening Fertility: The Essential Art of Preparing for PregnancyDe la EverandAwakening Fertility: The Essential Art of Preparing for PregnancyEvaluare: 4.5 din 5 stele4.5/5 (36)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouDe la EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouÎncă nu există evaluări
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeDe la EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeÎncă nu există evaluări
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenDe la EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenEvaluare: 4 din 5 stele4/5 (154)
- Perfectly Imperfect: Your complete guide to loving yourself and loving your bodyDe la EverandPerfectly Imperfect: Your complete guide to loving yourself and loving your bodyEvaluare: 5 din 5 stele5/5 (1)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodDe la EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodEvaluare: 4.5 din 5 stele4.5/5 (30)
- Labor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodDe la EverandLabor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodEvaluare: 4.5 din 5 stele4.5/5 (28)
- Spirit Baby: Communicate with Your Unborn Baby. Ease Your BirthDe la EverandSpirit Baby: Communicate with Your Unborn Baby. Ease Your BirthEvaluare: 5 din 5 stele5/5 (1)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainDe la EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainEvaluare: 4 din 5 stele4/5 (14)
- The Spark Factor: The Secret to Supercharging Energy, Becoming Resilient, and Feeling Better Than EverDe la EverandThe Spark Factor: The Secret to Supercharging Energy, Becoming Resilient, and Feeling Better Than EverEvaluare: 4 din 5 stele4/5 (2)
- Awakening Fertility: The Essential Art of Preparing for PregnancyDe la EverandAwakening Fertility: The Essential Art of Preparing for PregnancyEvaluare: 5 din 5 stele5/5 (4)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionDe la EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionEvaluare: 4.5 din 5 stele4.5/5 (124)
- Natural Hospital Birth: The Best of Both WorldsDe la EverandNatural Hospital Birth: The Best of Both WorldsEvaluare: 5 din 5 stele5/5 (33)
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfDe la EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfEvaluare: 5 din 5 stele5/5 (2)
- Rediscover Your Sparkle: Nourish Your SoulDe la EverandRediscover Your Sparkle: Nourish Your SoulEvaluare: 4.5 din 5 stele4.5/5 (4)
- Medical Bondage: Race, Gender, and the Origins of American GynecologyDe la EverandMedical Bondage: Race, Gender, and the Origins of American GynecologyEvaluare: 4.5 din 5 stele4.5/5 (75)
- The Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityDe la EverandThe Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityEvaluare: 4.5 din 5 stele4.5/5 (12)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondDe la EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondEvaluare: 4.5 din 5 stele4.5/5 (38)
- Menopause Confidential: A Doctor Reveals the Secrets to Thriving Through MidlifeDe la EverandMenopause Confidential: A Doctor Reveals the Secrets to Thriving Through MidlifeEvaluare: 4.5 din 5 stele4.5/5 (12)
- Menopause: All you need to know in one concise manualDe la EverandMenopause: All you need to know in one concise manualEvaluare: 5 din 5 stele5/5 (11)
- 9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthDe la Everand9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthÎncă nu există evaluări