S-ar putea să vă placă și
- AS Unit 1 Revision Note Physics IAL EdexcelDocument9 paginiAS Unit 1 Revision Note Physics IAL EdexcelMahbub Khan100% (1)
- Mastercard Foundation Scholars Program Application Form PDFDocument9 paginiMastercard Foundation Scholars Program Application Form PDFLanga SizibaÎncă nu există evaluări
- Hotel Berry Application FormDocument6 paginiHotel Berry Application Formmelissacorker100% (1)
- Affidavit of SeparationDocument1 paginăAffidavit of SeparationRaysunArellano100% (9)
- 39 Storey Treehouse Activity Pack PDFDocument11 pagini39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Synopsis On Employee LifecycleDocument12 paginiSynopsis On Employee LifecycleDeepak SinghÎncă nu există evaluări
- Free and Reduced Lunch ApplicationDocument2 paginiFree and Reduced Lunch Applicationhakone9027Încă nu există evaluări
- English 13-14 App and LTRDocument5 paginiEnglish 13-14 App and LTRapi-259143520Încă nu există evaluări
- Free Reduced AppDocument2 paginiFree Reduced ApplakeshoreshoriansÎncă nu există evaluări
- Income Eligibility Form For Family Day CareDocument4 paginiIncome Eligibility Form For Family Day Careapi-158762543Încă nu există evaluări
- Eskwela Davao Application FormDocument2 paginiEskwela Davao Application FormOhTenThicke100% (3)
- Combined Enrollment PacketDocument9 paginiCombined Enrollment PacketJustin FXÎncă nu există evaluări
- Aimhighapp 2015Document5 paginiAimhighapp 2015api-290166419Încă nu există evaluări
- JR High 2010 Registration FormDocument4 paginiJR High 2010 Registration FormryanlashleeÎncă nu există evaluări
- All Questions Must Be Answered, Incomplete Applications Will Not Be Considered!Document3 paginiAll Questions Must Be Answered, Incomplete Applications Will Not Be Considered!Arely CaroÎncă nu există evaluări
- KPC Inuka Scholarship Application Form 2024Document7 paginiKPC Inuka Scholarship Application Form 202420goldfinch301Încă nu există evaluări
- Eskwela Davao Application Form (Blank)Document2 paginiEskwela Davao Application Form (Blank)Aljeania Marie M. MolialÎncă nu există evaluări
- Eskwela Davao Application Form (Blank)Document2 paginiEskwela Davao Application Form (Blank)no one33% (3)
- Youth Ambassadors - Inbound Student Application - 2020 PDFDocument15 paginiYouth Ambassadors - Inbound Student Application - 2020 PDFDalilah CarpenterÎncă nu există evaluări
- 101652-Appendix B - Parents, Guardians or Sponsors 2017-18 2Document4 pagini101652-Appendix B - Parents, Guardians or Sponsors 2017-18 2allen.solorzano57Încă nu există evaluări
- Application For AssistanceDocument13 paginiApplication For Assistanceapi-242882048Încă nu există evaluări
- Nacac Application Fee WaiverDocument1 paginăNacac Application Fee Waiverapi-247039222Încă nu există evaluări
- Food Stamp App - stateAL'09Document3 paginiFood Stamp App - stateAL'09KJBATES389Încă nu există evaluări
- IwZaUmhI Application-Form PDFDocument2 paginiIwZaUmhI Application-Form PDFJaypee MartinÎncă nu există evaluări
- Morning ProgramDocument5 paginiMorning ProgramOrtizÎncă nu există evaluări
- Asmph Financial Aid Application - Non Ofw Income - Sy2013-14 PDFDocument19 paginiAsmph Financial Aid Application - Non Ofw Income - Sy2013-14 PDFCardioTCSÎncă nu există evaluări
- All Questions Must Be Answered, Incomplete Applications Will Not Be Considered!Document3 paginiAll Questions Must Be Answered, Incomplete Applications Will Not Be Considered!Arely CaroÎncă nu există evaluări
- Covid-19 Cares Act Funding Rental and Utility Assistance: Am I Eligible To Apply For This Assistance?Document11 paginiCovid-19 Cares Act Funding Rental and Utility Assistance: Am I Eligible To Apply For This Assistance?cory.mccooeyeÎncă nu există evaluări
- 2011-2012 Verification Form For Federal Student Aid ProgramsDocument3 pagini2011-2012 Verification Form For Federal Student Aid ProgramsKyle FalconerÎncă nu există evaluări
- Client Intake Form: (Last) (First) (MI)Document20 paginiClient Intake Form: (Last) (First) (MI)Prabha Gupta0% (1)
- (Contracting Entity Name) :, 2015-2016 Multi-Use Application For Free and Reduced-Price School MealsDocument3 pagini(Contracting Entity Name) :, 2015-2016 Multi-Use Application For Free and Reduced-Price School MealsCindyÎncă nu există evaluări
- Family Application Form: Please Print ClearlyDocument9 paginiFamily Application Form: Please Print ClearlyJulie Lyles CarrÎncă nu există evaluări
- Asmph Fa Application - New Student - 2015-16 FinalDocument45 paginiAsmph Fa Application - New Student - 2015-16 FinalKayle IrahÎncă nu există evaluări
- Doctor Statement Ssa 787Document3 paginiDoctor Statement Ssa 787Richard GuthÎncă nu există evaluări
- Gauteng Dept of Health Bursary Application FormDocument4 paginiGauteng Dept of Health Bursary Application FormLerato bunnyÎncă nu există evaluări
- Loh 2012 PDFDocument7 paginiLoh 2012 PDFJulie Lyles CarrÎncă nu există evaluări
- 2022-2023 Income and Expenses WorksheetDocument2 pagini2022-2023 Income and Expenses WorksheetDesy SelawatiÎncă nu există evaluări
- Dube Trade Port Application FormDocument7 paginiDube Trade Port Application FormNcediswaÎncă nu există evaluări
- Dressage Club AppDocument1 paginăDressage Club AppCyndie PittmanÎncă nu există evaluări
- Income Withholding For SupportDocument3 paginiIncome Withholding For SupportballÎncă nu există evaluări
- 2011 2012 Financial Aid ApplicationDocument4 pagini2011 2012 Financial Aid ApplicationSescily FeistyÎncă nu există evaluări
- Application Fee WaiverDocument1 paginăApplication Fee Waivermonee126Încă nu există evaluări
- Key-Club-Membership-Form 1Document4 paginiKey-Club-Membership-Form 1api-461627977Încă nu există evaluări
- Tzu Chi Scholarship Application Form (2023-2024)Document2 paginiTzu Chi Scholarship Application Form (2023-2024)Marjhie DionisioÎncă nu există evaluări
- DST EMBODI ApplicationDocument9 paginiDST EMBODI ApplicationMrs. LibbyÎncă nu există evaluări
- Go BIG For Parkinson Registration FormDocument2 paginiGo BIG For Parkinson Registration Formrickberry55Încă nu există evaluări
- Marital Separation Status AffidavitDocument2 paginiMarital Separation Status AffidavitRandy Sioson100% (1)
- Group Real Registration Form 1 - 3Document3 paginiGroup Real Registration Form 1 - 3api-259107792Încă nu există evaluări
- Tower Sacco Education Scholarship Form 2024Document9 paginiTower Sacco Education Scholarship Form 2024FOOTHILL CYBERÎncă nu există evaluări
- Request To Waive Repayment of Benefit Overpayment Balance: Statement of Financial ConditionDocument3 paginiRequest To Waive Repayment of Benefit Overpayment Balance: Statement of Financial Conditionangelalynnmartin4Încă nu există evaluări
- SCuEkVx3 Application-Form PDFDocument2 paginiSCuEkVx3 Application-Form PDFAlexis Stefannie RubionÎncă nu există evaluări
- 11-12 CCA Family Income FormDocument1 pagină11-12 CCA Family Income FormWilliena OwesÎncă nu există evaluări
- Cert Fin RespDocument2 paginiCert Fin Respapi-19509948Încă nu există evaluări
- Charity Care/Financial Assistance Application Form InstructionsDocument4 paginiCharity Care/Financial Assistance Application Form InstructionsDan SmithÎncă nu există evaluări
- Volunteer Registration Form Updated June 2021Document4 paginiVolunteer Registration Form Updated June 2021keamomalebe1Încă nu există evaluări
- Registration FormDocument2 paginiRegistration FormIris Auset ReidÎncă nu există evaluări
- FSA Motorola Stem ScholarshipDocument7 paginiFSA Motorola Stem Scholarshipdholland586Încă nu există evaluări
- Ad SupDocument2 paginiAd Supadamtefera.alxÎncă nu există evaluări
- State of Georgia Rental Assistance Program Income Documentation Waiver FormDocument2 paginiState of Georgia Rental Assistance Program Income Documentation Waiver FormSandra BenjaminÎncă nu există evaluări
- Description: Tags: FsDocument3 paginiDescription: Tags: Fsanon-5551Încă nu există evaluări
- Af Cavemen Cheer Try-Out PacketDocument5 paginiAf Cavemen Cheer Try-Out PacketAf CheerÎncă nu există evaluări
- Dss 8207 IaDocument10 paginiDss 8207 IaMaliÎncă nu există evaluări
- UNL Financial ResourceDocument2 paginiUNL Financial ResourceKofi AmoakoÎncă nu există evaluări
- Progressive Health Care: Critical Health Care InformationDe la EverandProgressive Health Care: Critical Health Care InformationÎncă nu există evaluări
- Basketball Calendar 2015-2016Document4 paginiBasketball Calendar 2015-2016api-248185821Încă nu există evaluări
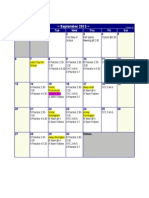
- Calendar of Events - SeptemberDocument1 paginăCalendar of Events - Septemberapi-248185821Încă nu există evaluări
- April Tucker Meets Her Goals As Sms Field Hockey CoachDocument1 paginăApril Tucker Meets Her Goals As Sms Field Hockey Coachapi-248185821Încă nu există evaluări
- Immunization LetterDocument1 paginăImmunization Letterapi-248185821Încă nu există evaluări
- NH Afterschool FactsDocument2 paginiNH Afterschool Factsapi-248185821Încă nu există evaluări
- EnrichmentsDocument3 paginiEnrichmentsapi-248185821Încă nu există evaluări
- 15 16 School Calendar Somersworth Approved 12 16 2014Document1 pagină15 16 School Calendar Somersworth Approved 12 16 2014api-248185821Încă nu există evaluări
- Volleyball 2015 CalendarDocument2 paginiVolleyball 2015 Calendarapi-248185821Încă nu există evaluări
- Field Hockey 2015 CalendarDocument2 paginiField Hockey 2015 Calendarapi-248185821Încă nu există evaluări
- Volleyball 2015 CalendarDocument2 paginiVolleyball 2015 Calendarapi-248185821Încă nu există evaluări
- Blood TestsDocument3 paginiBlood TestsMarycharinelle Antolin MolinaÎncă nu există evaluări
- Form Seven PlacementsDocument26 paginiForm Seven PlacementsRL Iroga100% (4)
- Comics Trip MasterpiecesDocument16 paginiComics Trip MasterpiecesDaniel Constantine100% (2)
- Questions & Answers: Webinar: Leveraging Caesar Ii and Featools Featuring PRGDocument8 paginiQuestions & Answers: Webinar: Leveraging Caesar Ii and Featools Featuring PRGMina MagdyÎncă nu există evaluări
- Docu69346 Unity Hybrid and Unity All Flash Configuring Converged Network Adaptor PortsDocument11 paginiDocu69346 Unity Hybrid and Unity All Flash Configuring Converged Network Adaptor PortsAmir Majzoub GhadiriÎncă nu există evaluări
- 9701 w19 QP 21 PDFDocument12 pagini9701 w19 QP 21 PDFFaiza KhalidÎncă nu există evaluări
- Fin - e - 178 - 2022-Covid AusterityDocument8 paginiFin - e - 178 - 2022-Covid AusterityMARUTHUPANDIÎncă nu există evaluări
- Case Study 1 - Whirlpool Reverser Logistics - With New Rubric - Winter 2022Document4 paginiCase Study 1 - Whirlpool Reverser Logistics - With New Rubric - Winter 2022ShravanÎncă nu există evaluări
- Tribebook Wendigo Revised Edition 6244638Document109 paginiTribebook Wendigo Revised Edition 6244638PedroÎncă nu există evaluări
- Youthful PopulationsDocument18 paginiYouthful PopulationsJamesy66Încă nu există evaluări
- Staedtler FIMO Catalogue 2019 (STAEDTLER Hobby Creative Catalogue 2019 En)Document100 paginiStaedtler FIMO Catalogue 2019 (STAEDTLER Hobby Creative Catalogue 2019 En)Tom S50% (2)
- HTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133Document3 paginiHTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133hadia duraniÎncă nu există evaluări
- Influence of Brand Experience On CustomerDocument16 paginiInfluence of Brand Experience On Customerarif adrianÎncă nu există evaluări
- đề thi TADocument15 paginiđề thi TAĐào Nguyễn Duy TùngÎncă nu există evaluări
- Mca Lawsuit Details English From 2007 To Feb 2021Document2 paginiMca Lawsuit Details English From 2007 To Feb 2021api-463871923Încă nu există evaluări
- The Honey Gatherers - Travels With The Bauls - The Wandering Minstrels of Rural India - Mimlu Sen PDFDocument16 paginiThe Honey Gatherers - Travels With The Bauls - The Wandering Minstrels of Rural India - Mimlu Sen PDFAurko F AhmadÎncă nu există evaluări
- QuizDocument15 paginiQuizGracie ChongÎncă nu există evaluări
- Ernieta - Entrep Survey Act.Document6 paginiErnieta - Entrep Survey Act.Nichole John ErnietaÎncă nu există evaluări
- Finals Lesson Ii Technology As A WAY of Revealing: Submitted By: Teejay M. AndrdaDocument8 paginiFinals Lesson Ii Technology As A WAY of Revealing: Submitted By: Teejay M. AndrdaTeejay AndradaÎncă nu există evaluări
- D245S 734046 Om enDocument90 paginiD245S 734046 Om enEndro Accoustic100% (1)
- 10 Ideas For ConversationDocument116 pagini10 Ideas For ConversationGreenLake36100% (1)
- Reflections: The Sol JournalDocument13 paginiReflections: The Sol Journalapi-268650070Încă nu există evaluări
- Practical No 4Document5 paginiPractical No 4Mahin SarkarÎncă nu există evaluări
- Test A 10 - 12520231610Document2 paginiTest A 10 - 12520231610Quang HuyÎncă nu există evaluări
- MCQ Class VDocument9 paginiMCQ Class VSneh MahajanÎncă nu există evaluări
- MEM Companion Volume Implementation Guide - Release 1.1Document23 paginiMEM Companion Volume Implementation Guide - Release 1.1Stanley AlexÎncă nu există evaluări