S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Solution Manual For Understanding Current Procedural Terminology and Hcpcs Coding Systems 6th Edition BowieDocument6 paginiSolution Manual For Understanding Current Procedural Terminology and Hcpcs Coding Systems 6th Edition BowieMrsElizabethHooveryspxw100% (85)
- Case Study On Pulmonary EmbolismDocument12 paginiCase Study On Pulmonary EmbolismJobelle Acena100% (2)
- Shouldice Hospital Case Study SolutionDocument10 paginiShouldice Hospital Case Study SolutionSambit Rath89% (9)
- DIN 1946-4 Engl. Dez. 2008Document68 paginiDIN 1946-4 Engl. Dez. 2008Lệ HoaÎncă nu există evaluări
- Diagnosis Icd X Tindakan Icd 9 CMDocument8 paginiDiagnosis Icd X Tindakan Icd 9 CMlinaÎncă nu există evaluări
- Application Form Birthing HomeDocument5 paginiApplication Form Birthing HomeKian AlfrzÎncă nu există evaluări
- Basketball Calendar 2015-2016Document4 paginiBasketball Calendar 2015-2016api-248185821Încă nu există evaluări
- Sms Welcome Back NewsletterDocument10 paginiSms Welcome Back Newsletterapi-248185821Încă nu există evaluări
- April Tucker Meets Her Goals As Sms Field Hockey CoachDocument1 paginăApril Tucker Meets Her Goals As Sms Field Hockey Coachapi-248185821Încă nu există evaluări
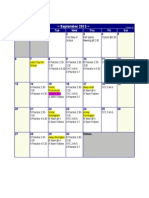
- Calendar of Events - SeptemberDocument1 paginăCalendar of Events - Septemberapi-248185821Încă nu există evaluări
- Immunization LetterDocument1 paginăImmunization Letterapi-248185821Încă nu există evaluări
- Scott Burrill3Document2 paginiScott Burrill3api-248185821Încă nu există evaluări
- HNH Grant Dental Care Flyer No Pull Tabs v2Document1 paginăHNH Grant Dental Care Flyer No Pull Tabs v2api-248185821Încă nu există evaluări
- NH Afterschool FactsDocument2 paginiNH Afterschool Factsapi-248185821Încă nu există evaluări
- Fall 2015 BrochureDocument2 paginiFall 2015 Brochureapi-248185821Încă nu există evaluări
- 15 16 School Calendar Somersworth Approved 12 16 2014Document1 pagină15 16 School Calendar Somersworth Approved 12 16 2014api-248185821Încă nu există evaluări
- EnrichmentsDocument3 paginiEnrichmentsapi-248185821Încă nu există evaluări
- Somersworth Middle School Student Hand Book 2015-2016Document38 paginiSomersworth Middle School Student Hand Book 2015-2016api-248185821Încă nu există evaluări
- Field Hockey 2015 CalendarDocument2 paginiField Hockey 2015 Calendarapi-248185821Încă nu există evaluări
- Soccer 2015 CalendarDocument2 paginiSoccer 2015 Calendarapi-248185821Încă nu există evaluări
- Residency AffidavitDocument2 paginiResidency Affidavitapi-248185821Încă nu există evaluări
- Volleyball 2015 CalendarDocument2 paginiVolleyball 2015 Calendarapi-248185821Încă nu există evaluări
- Volleyball 2015 CalendarDocument2 paginiVolleyball 2015 Calendarapi-248185821Încă nu există evaluări
- Sms Office 14110710050Document2 paginiSms Office 14110710050api-248185821Încă nu există evaluări
- Regristration PacketDocument9 paginiRegristration Packetapi-248185821Încă nu există evaluări
- Sms Office 14110710051Document1 paginăSms Office 14110710051api-248185821Încă nu există evaluări
- NSLP App Attach BDocument2 paginiNSLP App Attach Bapi-248185821Încă nu există evaluări
- Sheryl Ann M. Barreta: Position: Objective: Work ExperienceDocument3 paginiSheryl Ann M. Barreta: Position: Objective: Work ExperiencefayecolasÎncă nu există evaluări
- Second Year Clinical Posting Revised ScheduleDocument1 paginăSecond Year Clinical Posting Revised Schedulelove heartÎncă nu există evaluări
- PJO Jul-Dec 2011 Jan16 37-45 - Jose Rizal ArticleDocument9 paginiPJO Jul-Dec 2011 Jan16 37-45 - Jose Rizal ArticleMyRizal150Încă nu există evaluări
- Modern MedicineDocument6 paginiModern MedicinePenny FebriantiÎncă nu există evaluări
- Study Closely CT-MRIDocument3 paginiStudy Closely CT-MRITejas SawantÎncă nu există evaluări
- MBBS2014 SurgeryCaseAnalysisDocument194 paginiMBBS2014 SurgeryCaseAnalysisDaniel LimÎncă nu există evaluări
- Nursing Care For Patient Undergoing TAHBSO For Ovarian GrowthDocument4 paginiNursing Care For Patient Undergoing TAHBSO For Ovarian GrowthAyaBasilio100% (2)
- WHO Surgical Safety Checklist: Sign in Sign OutDocument1 paginăWHO Surgical Safety Checklist: Sign in Sign OutYoevfa Al-FathÎncă nu există evaluări
- Government Support Policy of Cosmetic Surgery Tourism in South Korea - GIM 2011 FINAL - For PresentationDocument34 paginiGovernment Support Policy of Cosmetic Surgery Tourism in South Korea - GIM 2011 FINAL - For PresentationNisanart Thadabusapa100% (2)
- Sr. No. Cghs Treatment Procedure/Investigation List (Delhi/Ncr) Non-Nabh/No Nabh/Nabl Rates Cghs Chennai Rate List 2014Document55 paginiSr. No. Cghs Treatment Procedure/Investigation List (Delhi/Ncr) Non-Nabh/No Nabh/Nabl Rates Cghs Chennai Rate List 2014Jaidilip JÎncă nu există evaluări
- Tugas Bahasa InggrisDocument2 paginiTugas Bahasa InggrisChennulÎncă nu există evaluări
- Intergroup Phase III RCT On Unresectable Head and Neck CancersDocument7 paginiIntergroup Phase III RCT On Unresectable Head and Neck CancersjmbobitÎncă nu există evaluări
- Bhang A Nada 1983Document7 paginiBhang A Nada 1983Teja LaksanaÎncă nu există evaluări
- Outcomes of Colorectal Surgery CRS at Department of Surgical Gastroenterology Max Hospital Saket InteDocument3 paginiOutcomes of Colorectal Surgery CRS at Department of Surgical Gastroenterology Max Hospital Saket InteGI Cancer IndiaÎncă nu există evaluări
- NURS 452 RCA2 Exemplar - Spring 2021Document11 paginiNURS 452 RCA2 Exemplar - Spring 2021Bryan NguyenÎncă nu există evaluări
- MATERI HAND HIGYNE DR - AhmadDocument40 paginiMATERI HAND HIGYNE DR - AhmadAhmad Dailah SudrajatÎncă nu există evaluări
- Perioperative Pathways Enhanced Recovery After SurgeryDocument11 paginiPerioperative Pathways Enhanced Recovery After SurgeryRIJANTOÎncă nu există evaluări
- MalpracticeDocument5 paginiMalpracticechris_awesomeÎncă nu există evaluări
- Integrative Final DraftDocument16 paginiIntegrative Final Draftapi-532928007Încă nu există evaluări
- Ventral HerniaDocument4 paginiVentral HerniaCristinaMadalinaÎncă nu există evaluări
- Medical Treatment of Battle WoundsDocument6 paginiMedical Treatment of Battle Woundskatgirl999Încă nu există evaluări
- Saudi J Anaesth 2013 7 1 57 60-TerkunciDocument4 paginiSaudi J Anaesth 2013 7 1 57 60-TerkunciRafael BagusÎncă nu există evaluări
- Hand Surgery PDFDocument36 paginiHand Surgery PDFkesjanaÎncă nu există evaluări
- Perioperative Teamwork For The Patient With A Shared AirwayDocument7 paginiPerioperative Teamwork For The Patient With A Shared AirwaysondiÎncă nu există evaluări