S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- LGBTQ Resource GuideDocument2 paginiLGBTQ Resource Guideapi-256935407Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Community OrganizationsDocument3 paginiCommunity Organizationsapi-256935407Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Self-Esteem Group PlansDocument13 paginiSelf-Esteem Group Plansapi-256935407Încă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
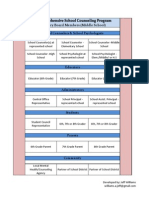
- Advisory Board General Mock UpDocument1 paginăAdvisory Board General Mock Upapi-256935407Încă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Ohio S Options For A High School DiplomaDocument30 paginiOhio S Options For A High School Diplomaapi-256935407Încă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Is Rules Mshs EngDocument1 paginăIs Rules Mshs Engapi-256935407Încă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Group Proposal Paper - The Changing Family GroupDocument11 paginiGroup Proposal Paper - The Changing Family Groupapi-256935407Încă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Mistaken Goal ChartDocument1 paginăMistaken Goal ChartvvaccountsÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- My Goal Poster 2Document1 paginăMy Goal Poster 2api-256935407Încă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Dev Theory OutlineDocument6 paginiDev Theory Outlineapi-256935407Încă nu există evaluări
- Gtky Dice Game Sheet1Document1 paginăGtky Dice Game Sheet1api-256935407Încă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Identity Development November 2014Document2 paginiIdentity Development November 2014api-256935407Încă nu există evaluări
- Resume 2014 WeeblyDocument2 paginiResume 2014 Weeblyapi-256935407Încă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Identity Development November 2014Document2 paginiIdentity Development November 2014api-256935407Încă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
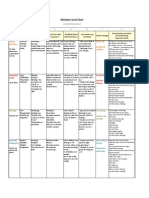
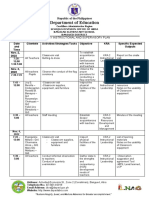
- Yearly Plan MemorialDocument2 paginiYearly Plan Memorialapi-256935407Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Identity Development November 2014Document2 paginiIdentity Development November 2014api-256935407Încă nu există evaluări
- Gradreq 2018Document1 paginăGradreq 2018api-256935407Încă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Gradreq 2018Document1 paginăGradreq 2018api-256935407Încă nu există evaluări
- Role of A School CounselorDocument2 paginiRole of A School Counselorapi-257858054Încă nu există evaluări
- Measure Assignment WilliamsDocument5 paginiMeasure Assignment Williamsapi-256935407Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Omj-K-12-Registration 4-2014Document19 paginiOmj-K-12-Registration 4-2014api-256935407Încă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Automation Industry PPT 2-3 ADocument16 paginiAutomation Industry PPT 2-3 AVijay Vj100% (1)
- TLE8 Nail Care First QuarterDocument6 paginiTLE8 Nail Care First QuarterGretchen Sarmiento Cabarles AlbaoÎncă nu există evaluări
- Interactions Between Rodent Visual and Spatial Systems During NavigationDocument15 paginiInteractions Between Rodent Visual and Spatial Systems During Navigation伟健宗Încă nu există evaluări
- Camp Elizabeth ImaginationDocument24 paginiCamp Elizabeth ImaginationSandraVisokolskisÎncă nu există evaluări
- First Class English For It 1° ClassDocument19 paginiFirst Class English For It 1° ClassPame WernliÎncă nu există evaluări
- Influences of Product Attributes and Lifestyles On Consumer Behavior - A Case Study of Coffee Consumption in IndonesiaDocument12 paginiInfluences of Product Attributes and Lifestyles On Consumer Behavior - A Case Study of Coffee Consumption in IndonesiaVeronica Yjah Canlaon ÑazqueÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- EMS Leadership For New EMTsDocument53 paginiEMS Leadership For New EMTsBethuel Aliwa100% (1)
- Week 10 11 System Dynamics Using-Powersim Studio 2005Document55 paginiWeek 10 11 System Dynamics Using-Powersim Studio 2005Hawa Aqmarina Zen PutriÎncă nu există evaluări
- English Unit 4 Draft TG PDFDocument94 paginiEnglish Unit 4 Draft TG PDFAnime AddictÎncă nu există evaluări
- Different Kinds of SpeechDocument2 paginiDifferent Kinds of SpeechMaridel SulbianoÎncă nu există evaluări
- Unit #4 Grade Topic Title Subject(s) Unit Guiding Questions: Energize Me 6Document8 paginiUnit #4 Grade Topic Title Subject(s) Unit Guiding Questions: Energize Me 6shaneearlÎncă nu există evaluări
- Oc Module-5Document13 paginiOc Module-5Stephanie Nichole Ian CasemÎncă nu există evaluări
- Eng PWPDocument3 paginiEng PWPNonthakorn Pornpaisansakul0% (1)
- Certificate of Originality: Place: Place: Date: DateDocument4 paginiCertificate of Originality: Place: Place: Date: DateSumit PandeyÎncă nu există evaluări
- Information Theory and Coding PDFDocument214 paginiInformation Theory and Coding PDFMohan Raj100% (1)
- Workbook For How To Grow A Connected FamilyDocument65 paginiWorkbook For How To Grow A Connected FamilyPenny PedenÎncă nu există evaluări
- NLC23 - Grade 7 Enhancement Mathematics Lesson Plan - FinalDocument64 paginiNLC23 - Grade 7 Enhancement Mathematics Lesson Plan - FinalJohn Christopher Romero100% (2)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Assessment Task 3 - BSBINN502Document12 paginiAssessment Task 3 - BSBINN502meht firsatÎncă nu există evaluări
- SST Lesson PlanDocument3 paginiSST Lesson Planapi-540108167Încă nu există evaluări
- King - Template AnalysisDocument24 paginiKing - Template AnalysisAnita Johnson75% (4)
- Dissertation Topics Criminal PsychologyDocument5 paginiDissertation Topics Criminal PsychologyBuyingPapersOnlineCollegeSpringfield100% (1)
- Monthly Instructional and Supervisory PlanDocument6 paginiMonthly Instructional and Supervisory PlanTine CristineÎncă nu există evaluări
- Analysis of The Speech Acts in A Language Class EssayDocument4 paginiAnalysis of The Speech Acts in A Language Class EssayOscar López SerranoÎncă nu există evaluări
- ADJ Phrase 2Document13 paginiADJ Phrase 2scud_tienÎncă nu există evaluări
- ELS 133 - ApproachesDocument64 paginiELS 133 - ApproachesRJEREEÎncă nu există evaluări
- Session 1 Session 2 Session 3 Session 4: A. Content StandardDocument3 paginiSession 1 Session 2 Session 3 Session 4: A. Content StandardPrecious Gabrillo GabagatÎncă nu există evaluări
- Writing ObjectivesDocument22 paginiWriting ObjectiveswintermaeÎncă nu există evaluări
- Model Free Adaptive Predictive ControlDocument7 paginiModel Free Adaptive Predictive Controldee1985Încă nu există evaluări
- FINAL COACHING GOOD LUCK Let 2017Document177 paginiFINAL COACHING GOOD LUCK Let 2017Idris HermanÎncă nu există evaluări
- Lesson 3 Methods and Techniques in Teaching Araling PanlipunanDocument19 paginiLesson 3 Methods and Techniques in Teaching Araling PanlipunanAbellar Shania Cristine74% (31)
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesDe la EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesEvaluare: 5 din 5 stele5/5 (1635)
- Summary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearDe la EverandSummary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearEvaluare: 4.5 din 5 stele4.5/5 (560)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Power of Now: A Guide to Spiritual EnlightenmentDe la EverandThe Power of Now: A Guide to Spiritual EnlightenmentEvaluare: 4.5 din 5 stele4.5/5 (4125)