S-ar putea să vă placă și
- Enrollment FormDocument1 paginăEnrollment Formthinker03Încă nu există evaluări
- Athletic Information FormDocument5 paginiAthletic Information FormGino LudoviceÎncă nu există evaluări
- Ambassador Application FormDocument1 paginăAmbassador Application FormMi Llamo JaneÎncă nu există evaluări
- Sample Employment AppDocument2 paginiSample Employment AppjksongÎncă nu există evaluări
- MPDFDocument3 paginiMPDFKbÎncă nu există evaluări
- Bike Loan Application FormDocument1 paginăBike Loan Application FormRomel Solis MadiaÎncă nu există evaluări
- ApplicationDocument2 paginiApplicationGrace Deleeuw PelusoÎncă nu există evaluări
- Sustainer FormDocument1 paginăSustainer FormsypermathÎncă nu există evaluări
- Application For Employment For Office Use OnlyDocument9 paginiApplication For Employment For Office Use OnlyMr. PicklesÎncă nu există evaluări
- Highland Rental Application PDFDocument2 paginiHighland Rental Application PDFMike CrakerÎncă nu există evaluări
- Mau Don Xin Viec Ngan HanDocument3 paginiMau Don Xin Viec Ngan HanalseriÎncă nu există evaluări
- FormDocument4 paginiFormAble K-HeavenÎncă nu există evaluări
- Medical FormDocument1 paginăMedical FormCarolinasCKIÎncă nu există evaluări
- 4H Adult Enrollment FormDocument2 pagini4H Adult Enrollment FormJCSÎncă nu există evaluări
- Scholarship FormDocument3 paginiScholarship Formyaranaser246Încă nu există evaluări
- Patient Feedback CardDocument2 paginiPatient Feedback Cardapi-459076195Încă nu există evaluări
- Pre Application FomDocument2 paginiPre Application FomLindelane Lee Praise MavimbelaÎncă nu există evaluări
- Internship ApplicationDocument4 paginiInternship Applicationapi-124861674Încă nu există evaluări
- Bandera AppDocument4 paginiBandera AppJuana EscamillaÎncă nu există evaluări
- Exit Paper 3Document2 paginiExit Paper 3Catherine De LunaÎncă nu există evaluări
- New Patient FormDocument8 paginiNew Patient Forme-MedTools100% (5)
- Volunteer Application 2012Document2 paginiVolunteer Application 2012api-205814442Încă nu există evaluări
- KZN COGTA Bursary Application Form 2024Document7 paginiKZN COGTA Bursary Application Form 2024thabisileÎncă nu există evaluări
- FundagreementnewDocument6 paginiFundagreementnewapi-340041361Încă nu există evaluări
- Application For Admission EditDocument5 paginiApplication For Admission EditRhonDaleRedCabreraÎncă nu există evaluări
- Bellport Bay Yacht ClubDocument2 paginiBellport Bay Yacht Clubbitch fÎncă nu există evaluări
- Who Wants To Be A Millionaire ApplicationDocument4 paginiWho Wants To Be A Millionaire Applicationkhani.naser8834Încă nu există evaluări
- Employment HistoryDocument1 paginăEmployment HistorydeviascoÎncă nu există evaluări
- Fuel Gladiators Permission SlipDocument1 paginăFuel Gladiators Permission Slipjoebel105Încă nu există evaluări
- Youth Profile Form With Letter HeadDocument2 paginiYouth Profile Form With Letter HeadLyca Marie CerezaÎncă nu există evaluări
- KwaZulu Natal Department of Transport Bursary Application FormDocument8 paginiKwaZulu Natal Department of Transport Bursary Application FormMandisa ZibulaÎncă nu există evaluări
- Simon Application SetDocument23 paginiSimon Application SetRobert TruongÎncă nu există evaluări
- LIFE PROJECT 8th GRADEDocument13 paginiLIFE PROJECT 8th GRADEJose Fernando Arango PalacioÎncă nu există evaluări
- Life School Input SheetDocument1 paginăLife School Input Sheetapi-3703184Încă nu există evaluări
- 2015 Scholarship ApplicationDocument3 pagini2015 Scholarship Applicationapi-280767644Încă nu există evaluări
- Bikram Chowk, Jammu: Amar Singh Club (Regd.)Document3 paginiBikram Chowk, Jammu: Amar Singh Club (Regd.)kaminiÎncă nu există evaluări
- Exploration WrksheetsDocument24 paginiExploration WrksheetsAideen O'SullivanÎncă nu există evaluări
- Notes: Face AmountDocument4 paginiNotes: Face Amountqris24Încă nu există evaluări
- CCI Student ApplicationDocument4 paginiCCI Student ApplicationIbrahim KalokohÎncă nu există evaluări
- WOW Kid's Club Health FormDocument4 paginiWOW Kid's Club Health FormKetron Memorial United Methodist ChurchÎncă nu există evaluări
- DateDocument4 paginiDateapi-26391568Încă nu există evaluări
- Applicant Application FormDocument6 paginiApplicant Application FormJocelyn Joy ArcegaÎncă nu există evaluări
- End of Semester Report: PhilanthropyDocument3 paginiEnd of Semester Report: PhilanthropyIbrahim SalahudinÎncă nu există evaluări
- Domestic Grad Admission ApplicationDocument2 paginiDomestic Grad Admission ApplicationEmmanuella Feudjio WambaÎncă nu există evaluări
- Qat Form C 1Document3 paginiQat Form C 1Seanjames JacobÎncă nu există evaluări
- Senior Brag SheetDocument3 paginiSenior Brag Sheetapi-307211076Încă nu există evaluări
- Jms FormDocument1 paginăJms Formabdul haqÎncă nu există evaluări
- Signature of Delegation Signature of Candidate Signature of JMSDocument1 paginăSignature of Delegation Signature of Candidate Signature of JMSAlishahÎncă nu există evaluări
- Elections Commission ApplicationDocument2 paginiElections Commission ApplicationKUStudentSenateÎncă nu există evaluări
- University of Kansas Elections Commission Application 2013Document2 paginiUniversity of Kansas Elections Commission Application 2013KUStudentSenateÎncă nu există evaluări
- Subject & Schedule: - Group Activity No. - TitleDocument2 paginiSubject & Schedule: - Group Activity No. - TitleEmmanuel Jimenez-Bacud, CSE-Professional,BA-MA Pol SciÎncă nu există evaluări
- BNG7 Qybz RD9 QXQ 3 V WR 3 VX RDocument5 paginiBNG7 Qybz RD9 QXQ 3 V WR 3 VX Rkudzaishe mhereÎncă nu există evaluări
- Centennial International Education - Loyalty Scholarship ApplicationDocument2 paginiCentennial International Education - Loyalty Scholarship ApplicationVeronica PontesÎncă nu există evaluări
- Scholarship ApplicationDocument3 paginiScholarship ApplicationgeneraljoeÎncă nu există evaluări
- Personnel Information Sheet (New) PDFDocument5 paginiPersonnel Information Sheet (New) PDFLoo PeaÎncă nu există evaluări
- The Exchange The Exchange Profile Sheet: ALTAR, Catherine Sienna B. BSN Ii-D 180777 Phihum-DDocument1 paginăThe Exchange The Exchange Profile Sheet: ALTAR, Catherine Sienna B. BSN Ii-D 180777 Phihum-DsenyorakathÎncă nu există evaluări
- Franchise Application FormDocument13 paginiFranchise Application FormBart KosongtujuhÎncă nu există evaluări
- The Honest and Direct Truth to Resumes from an HR Director PerspectiveDe la EverandThe Honest and Direct Truth to Resumes from an HR Director PerspectiveÎncă nu există evaluări
- Progressive Health Care: Critical Health Care InformationDe la EverandProgressive Health Care: Critical Health Care InformationÎncă nu există evaluări
- Last Christmas - MelodiDocument2 paginiLast Christmas - MelodiAdamÎncă nu există evaluări
- Orla Us Letter Paper PDFDocument25 paginiOrla Us Letter Paper PDFAsif K100% (2)
- Fourth Quarterly Test in Mathematics 6Document4 paginiFourth Quarterly Test in Mathematics 6Cher An JieÎncă nu există evaluări
- 01 To 15 AUGUST GAURAV BHAI DAILY PDFDocument508 pagini01 To 15 AUGUST GAURAV BHAI DAILY PDFrupaÎncă nu există evaluări
- Advances in FunctionalDocument287 paginiAdvances in FunctionalLynsey100% (1)
- Types of EventsDocument6 paginiTypes of EventsBernalyn ManaogÎncă nu există evaluări
- Official Dreamcast Magazine PDFDocument2 paginiOfficial Dreamcast Magazine PDFChantelÎncă nu există evaluări
- Karate Grading - Manual PDFDocument25 paginiKarate Grading - Manual PDFincredibletpÎncă nu există evaluări
- Barefoot Earthing (OnFitness Magazine)Document4 paginiBarefoot Earthing (OnFitness Magazine)JohanÎncă nu există evaluări
- Mens Health October 2016 UK PDFDocument226 paginiMens Health October 2016 UK PDFAj YangÎncă nu există evaluări
- A Folklore Bestiary For 5E and OSE by Olivier Revenu - KickstarterDocument1 paginăA Folklore Bestiary For 5E and OSE by Olivier Revenu - KickstarterTesting0% (3)
- Collective Past Board Exam Questionnaire (PROFESSIONAL PRACTICE)Document5 paginiCollective Past Board Exam Questionnaire (PROFESSIONAL PRACTICE)Erwin AriolaÎncă nu există evaluări
- CZ 75 Kadet: Instruction ManualDocument0 paginiCZ 75 Kadet: Instruction Manualab212amisarÎncă nu există evaluări
- Part Catalogue Yamaha YZF R25 2020 B4P1 MALAYSIADocument69 paginiPart Catalogue Yamaha YZF R25 2020 B4P1 MALAYSIAmhz myÎncă nu există evaluări
- Wipro14thjulychd, Sms SentDocument236 paginiWipro14thjulychd, Sms SentAnup ChhabraÎncă nu există evaluări
- Highway Code PDFDocument189 paginiHighway Code PDFjhaider20009Încă nu există evaluări
- Colombiaf 1Document1 paginăColombiaf 1Alonso Pahuacho PortellaÎncă nu există evaluări
- Wing Chun TestingDocument9 paginiWing Chun TestingIan100% (1)
- Wheel AlignmentDocument4 paginiWheel AlignmentdonlynÎncă nu există evaluări
- T 606 PG 157-160 PDFDocument4 paginiT 606 PG 157-160 PDFJossimar PerezÎncă nu există evaluări
- Easy EKGDocument45 paginiEasy EKGnov14Încă nu există evaluări
- Marion County Public SchoolsDocument1 paginăMarion County Public SchoolsWFTVÎncă nu există evaluări
- Just Uploaded To DownloadDocument4 paginiJust Uploaded To DownloadZachyboiÎncă nu există evaluări
- HikingDocument2 paginiHikingIanne Violet Yumierre TabañagÎncă nu există evaluări
- 8PofJezchP79UqAFZAba PDFDocument44 pagini8PofJezchP79UqAFZAba PDFSumant SharmaÎncă nu există evaluări
- Bi 187 Lecture 1Document24 paginiBi 187 Lecture 1michael6tan-1Încă nu există evaluări
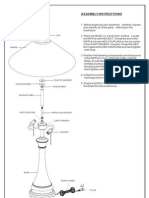
- Assembly Instructions: FinialDocument1 paginăAssembly Instructions: Finialdayshift5Încă nu există evaluări
- DPS Calculator - DRGDocument216 paginiDPS Calculator - DRGSmitty WerbenjagermanjensenÎncă nu există evaluări
- Fedor Emelianenko Fedor Emelianenko: The Last Emperor The Last EmperorDocument4 paginiFedor Emelianenko Fedor Emelianenko: The Last Emperor The Last EmperorznakizzÎncă nu există evaluări
- Port GameDocument9 paginiPort GameMamajokoÎncă nu există evaluări