S-ar putea să vă placă și
- Declaration Form by The Sponsoring Facility: Personal DetailsDocument1 paginăDeclaration Form by The Sponsoring Facility: Personal DetailsMohammed TazminullaÎncă nu există evaluări
- To, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New BusinessDocument1 paginăTo, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New Businessdharam singhÎncă nu există evaluări
- Hipaa 1Document1 paginăHipaa 1Gregory KnispelÎncă nu există evaluări
- Patient Information Sheet 091409Document2 paginiPatient Information Sheet 091409api-16816262Încă nu există evaluări
- Personal Information SheetDocument3 paginiPersonal Information SheetPaula ValerioÎncă nu există evaluări
- Hipaa Release Form FloridaDocument3 paginiHipaa Release Form FloridaAlan WattsÎncă nu există evaluări
- HDFC Life policy name declaration documentDocument1 paginăHDFC Life policy name declaration documentHarsh ParmarÎncă nu există evaluări
- Customer Mandate Cum Declaration Form For New Business: Shriram Life Insurance Company LimitedDocument1 paginăCustomer Mandate Cum Declaration Form For New Business: Shriram Life Insurance Company LimitedShashank DixitÎncă nu există evaluări
- Adult NP Ppwrork KCPGDocument16 paginiAdult NP Ppwrork KCPGMary GreerÎncă nu există evaluări
- TEMPLATE Etiqa Out Patient Claim FormDocument1 paginăTEMPLATE Etiqa Out Patient Claim FormEvoy EstradaÎncă nu există evaluări
- Etiqa Out Patient Claim FormDocument1 paginăEtiqa Out Patient Claim FormAlmecestrisÎncă nu există evaluări
- Us Health - Care - Proxy - FormDocument3 paginiUs Health - Care - Proxy - Form健康生活園Healthy Life GardenÎncă nu există evaluări
- CDF - CCD For HsecDocument1 paginăCDF - CCD For HsecNishanth VarmaÎncă nu există evaluări
- Health Fair Invitation - Promote Wellness to EmployeesDocument1 paginăHealth Fair Invitation - Promote Wellness to Employeesaamer141100% (1)
- Patient RegistrationDocument2 paginiPatient RegistrationrehbergÎncă nu există evaluări
- SPC - Intake Form and POA Requires NotaryDocument2 paginiSPC - Intake Form and POA Requires NotaryVanessa Collins SimmsÎncă nu există evaluări
- Checklist Grant For Wholesale Drug License PDFDocument11 paginiChecklist Grant For Wholesale Drug License PDFShwetank SinghÎncă nu există evaluări
- Empire Document ApplicationDocument9 paginiEmpire Document Applicationapi-253439645Încă nu există evaluări
- DRUG TESTING CONSENT TITLEDocument7 paginiDRUG TESTING CONSENT TITLEShawn JordanÎncă nu există evaluări
- PDS CS Form No 212 Revised2017Document7 paginiPDS CS Form No 212 Revised2017Buddy BuzzÎncă nu există evaluări
- Advocare Consent Disclosure Authorization PDFDocument2 paginiAdvocare Consent Disclosure Authorization PDFAsnaifa Bint MamintalÎncă nu există evaluări
- Proposal Form For Loss of Licence & Personal Accident PolicyDocument2 paginiProposal Form For Loss of Licence & Personal Accident PolicyrajmercuryÎncă nu există evaluări
- Patient Demographics 12-12-12Document4 paginiPatient Demographics 12-12-12api-233056868Încă nu există evaluări
- Clinical Referral FormDocument2 paginiClinical Referral FormJan Oneille Y. VallesÎncă nu există evaluări
- Business Loan Application Form: DD MM YyyyDocument8 paginiBusiness Loan Application Form: DD MM YyyyNilesh FalmariÎncă nu există evaluări
- Application For Wholesale MedicineDocument8 paginiApplication For Wholesale Medicinesashi debsarmaÎncă nu există evaluări
- Proposal form for loss of licence & personal accident policyDocument2 paginiProposal form for loss of licence & personal accident policyVijay SinghÎncă nu există evaluări
- Registration form for vibration analysis workshopDocument2 paginiRegistration form for vibration analysis workshopJobyThomasIssacÎncă nu există evaluări
- Sample Consent 2020 Update FinalDocument1 paginăSample Consent 2020 Update FinalKevin G. DavisÎncă nu există evaluări
- Loan Application FormDocument2 paginiLoan Application FormDean DanaiÎncă nu există evaluări
- GTI-Claim-Form - (Employer - Employee)Document3 paginiGTI-Claim-Form - (Employer - Employee)priyanshusharma8840Încă nu există evaluări
- Agents ApplicationDocument6 paginiAgents ApplicationRamananÎncă nu există evaluări
- Tac Appendix 6Document1 paginăTac Appendix 6Anbaraj Arun100% (1)
- Commitment LetterDocument1 paginăCommitment LetterAbdul HannanÎncă nu există evaluări
- HEALTH CLAIM FORMDocument4 paginiHEALTH CLAIM FORMCharles RodriguesÎncă nu există evaluări
- Credit ApplicationDocument3 paginiCredit ApplicationHeather Snyder CherroneÎncă nu există evaluări
- HMO Accreditation FormDocument1 paginăHMO Accreditation FormGenesis LazargaÎncă nu există evaluări
- The Following Deposits Are Required To Be Paid by Clients Immediately After Bank EndorsementDocument29 paginiThe Following Deposits Are Required To Be Paid by Clients Immediately After Bank EndorsementEnrique RiveraÎncă nu există evaluări
- Health Care Proxy Form - EnglishDocument2 paginiHealth Care Proxy Form - EnglishTheFloatingHospitalÎncă nu există evaluări
- Beneficial Ownership DeclarationDocument2 paginiBeneficial Ownership Declarationonly4zbackupÎncă nu există evaluări
- Loan Application FormDocument2 paginiLoan Application FormLewis Livestre, Jr.Încă nu există evaluări
- Limited Power of AttorneyDocument5 paginiLimited Power of AttorneyKrite BanggawanÎncă nu există evaluări
- FDA Philippines Cosmetic Business AffidavitDocument2 paginiFDA Philippines Cosmetic Business AffidavitOmar AsodisenÎncă nu există evaluări
- Application For Admission: Personal DetailsDocument3 paginiApplication For Admission: Personal DetailsRaza YaseenÎncă nu există evaluări
- Philippine Survey ApplicationDocument2 paginiPhilippine Survey ApplicationEdcel SilvaÎncă nu există evaluări
- Authorisation LetterDocument2 paginiAuthorisation LetterAnand KhotÎncă nu există evaluări
- Business Loan Application Form IDFC BankDocument8 paginiBusiness Loan Application Form IDFC BankSÎncă nu există evaluări
- Sample HIE Consent 2020 Update FinalDocument1 paginăSample HIE Consent 2020 Update FinalKevin G. DavisÎncă nu există evaluări
- Annexure - A Declaration of Beneficial OwnershipDocument2 paginiAnnexure - A Declaration of Beneficial OwnershipSHASHI KANT75% (4)
- Offices InstitutionsDocument1 paginăOffices InstitutionsMECHSTER mechsterÎncă nu există evaluări
- Client Information SheetDocument1 paginăClient Information SheetAnonymous Nw6c3H0Încă nu există evaluări
- PPR 2015 - Training Form PDFDocument2 paginiPPR 2015 - Training Form PDFShreejayaÎncă nu există evaluări
- Gratuity Form-IDocument3 paginiGratuity Form-IanupamaÎncă nu există evaluări
- CONSENT TO DISCLOSE PERSONAL INFORMATIONDocument2 paginiCONSENT TO DISCLOSE PERSONAL INFORMATIONRowell VillanuevaÎncă nu există evaluări
- Male New Patient Paperwork 5.2015Document8 paginiMale New Patient Paperwork 5.2015Muhammad AdeelÎncă nu există evaluări
- Complaint FormDocument4 paginiComplaint FormAlan WattsÎncă nu există evaluări
- SX Account Authorization Form - Primary Contact (01-25-2018) PDFDocument1 paginăSX Account Authorization Form - Primary Contact (01-25-2018) PDFJoseph PoreÎncă nu există evaluări
- IA Hartford Indemnity AgreementDocument1 paginăIA Hartford Indemnity AgreementDënnis DukeÎncă nu există evaluări
- KYC FormDocument2 paginiKYC FormTilottoma NathÎncă nu există evaluări
- Medical Equipment and Supply Business: Your Multi Billion Dollar Guide to Start-UpDe la EverandMedical Equipment and Supply Business: Your Multi Billion Dollar Guide to Start-UpÎncă nu există evaluări
- STUDENT LINKING WORDS AND PHRASESDocument6 paginiSTUDENT LINKING WORDS AND PHRASESEdward YooÎncă nu există evaluări
- Difference BTW False, No, NGDocument1 paginăDifference BTW False, No, NGDr-Usman KhanÎncă nu există evaluări
- IELTS Writing Answer SheetDocument4 paginiIELTS Writing Answer SheetHighPoint IELTS Preparation Services, Inc.Încă nu există evaluări
- Speaking Tips by RyanDocument2 paginiSpeaking Tips by RyanDr-Usman Khan100% (3)
- YES-IELTS - Decoding The IELTS Band Descriptors - Writing Task 2 - Task Response - Bands 6, 7, 8, 9Document6 paginiYES-IELTS - Decoding The IELTS Band Descriptors - Writing Task 2 - Task Response - Bands 6, 7, 8, 9YES IELTS100% (2)
- IELTS True False Not GivenDocument5 paginiIELTS True False Not GivenDr-Usman Khan100% (2)
- IELTS Speaking Part 1 VocabularyDocument24 paginiIELTS Speaking Part 1 VocabularyDr-Usman Khan100% (1)
- Difference BTW False, No, NGDocument1 paginăDifference BTW False, No, NGDr-Usman KhanÎncă nu există evaluări
- Exam MaterialsDocument4 paginiExam MaterialsDr-Usman KhanÎncă nu există evaluări
- TransitionsDocument3 paginiTransitionsDr-Usman KhanÎncă nu există evaluări
- Essay Question 1 - Outsourcing Labour Related Work To Poorer Nations - Corrected by RyanDocument5 paginiEssay Question 1 - Outsourcing Labour Related Work To Poorer Nations - Corrected by RyanDr-Usman Khan0% (1)
- PharmaciesDocument18 paginiPharmaciesDr-Usman KhanÎncă nu există evaluări
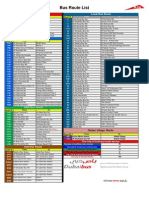
- Bus Route List EnglishDocument1 paginăBus Route List EnglishDr-Usman KhanÎncă nu există evaluări
- Connectors For IELTSDocument24 paginiConnectors For IELTSDr-Usman KhanÎncă nu există evaluări
- Nol 7zone Eng PDFDocument1 paginăNol 7zone Eng PDFneedzinÎncă nu există evaluări
- 30-01-2014 Test Malik Asif Javaid AwanDocument4 pagini30-01-2014 Test Malik Asif Javaid AwanDr-Usman Khan67% (3)
- Bus Route List EnglishDocument1 paginăBus Route List EnglishDr-Usman KhanÎncă nu există evaluări
- 32 Ielts Essay Samples Band 9Document34 pagini32 Ielts Essay Samples Band 9mh73% (26)
- 570 Academic Word List For IELTSDocument26 pagini570 Academic Word List For IELTSXanh Lè100% (1)
- 06 MarchDocument3 pagini06 MarchDr-Usman Khan0% (1)
- 23 QsDocument8 pagini23 QsDr-Usman Khan0% (1)
- The Drugs Act, 1976Document32 paginiThe Drugs Act, 1976Dr-Usman KhanÎncă nu există evaluări
- Dha Prometric Feb-3 ShabeerDocument2 paginiDha Prometric Feb-3 ShabeerDr-Usman KhanÎncă nu există evaluări
- 5 2 2014 - 2Document2 pagini5 2 2014 - 2Dr-Usman Khan100% (1)
- Dha Prometric Feb-3 ShabeerDocument2 paginiDha Prometric Feb-3 ShabeerDr-Usman KhanÎncă nu există evaluări
- 5 2 2014 - 2Document2 pagini5 2 2014 - 2Dr-Usman Khan100% (1)
- DHA Prometric Exam 02-01-2014 Role of Carbidopa in ParkinsonismDocument4 paginiDHA Prometric Exam 02-01-2014 Role of Carbidopa in ParkinsonismDr-Usman Khan79% (14)
- Writing Task 1 1-8Document28 paginiWriting Task 1 1-8Dr-Usman KhanÎncă nu există evaluări
- Good CommunicationDocument6 paginiGood CommunicationKranthi KumarÎncă nu există evaluări