S-ar putea să vă placă și
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementDe la EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreÎncă nu există evaluări
- 630 Submitted Occupational Profile and AnalysisDocument21 pagini630 Submitted Occupational Profile and Analysisapi-310815315Încă nu există evaluări
- Occt630 Occupational Profile InterventionDocument19 paginiOcct630 Occupational Profile Interventionapi-290880850Încă nu există evaluări
- Occupational Profile M Viveros FinalDocument19 paginiOccupational Profile M Viveros Finalapi-293258738Încă nu există evaluări
- 630 Occupational Profile AssignmentDocument13 pagini630 Occupational Profile Assignmentapi-201999002Încă nu există evaluări
- Occupational Profile and Intervention PlanDocument13 paginiOccupational Profile and Intervention Planapi-251993533Încă nu există evaluări
- Occt 651 - Occupational Profile PaperDocument20 paginiOcct 651 - Occupational Profile Paperapi-293243330Încă nu există evaluări
- Occupational ProfileDocument21 paginiOccupational Profileapi-293223028100% (1)
- Occupational Profile Intervention PlanDocument17 paginiOccupational Profile Intervention Planapi-264481356Încă nu există evaluări
- Occt 630 - Occupational Profile and Intervention Plan - PortfolioDocument21 paginiOcct 630 - Occupational Profile and Intervention Plan - Portfolioapi-279916752Încă nu există evaluări
- Kristen Kincaid Occupational Analysis & Intervention PlanDocument23 paginiKristen Kincaid Occupational Analysis & Intervention Planapi-282525755100% (1)
- Eval Soap Note 2Document9 paginiEval Soap Note 2api-435763096Încă nu există evaluări
- 4th Sem 651 Occupational ProfileDocument19 pagini4th Sem 651 Occupational Profileapi-291545292100% (1)
- Occupational Profile and Intervention Plan FinalDocument21 paginiOccupational Profile and Intervention Plan Finalapi-293223028Încă nu există evaluări
- Running Head: Occupational Profile and Intervention Plan 1Document19 paginiRunning Head: Occupational Profile and Intervention Plan 1api-292735638Încă nu există evaluări
- Occt 651 - Occupational Profile and Intervention PlanDocument22 paginiOcct 651 - Occupational Profile and Intervention Planapi-279916752Încă nu există evaluări
- Initial TemplateDocument8 paginiInitial TemplateZuj PayÎncă nu există evaluări
- Dick, Elisa - Occupational ProfileDocument10 paginiDick, Elisa - Occupational Profileapi-234536968Încă nu există evaluări
- Occupational Analysis Intervention Plan PDFDocument20 paginiOccupational Analysis Intervention Plan PDFapi-293182319Încă nu există evaluări
- Artifact 5 Soap NoteDocument3 paginiArtifact 5 Soap Noteapi-517998988Încă nu există evaluări
- Ashley M Occt 651 Occupational ProfileDocument11 paginiAshley M Occt 651 Occupational Profileapi-25080062950% (2)
- Occupational Profile and Intervention Plan FinalDocument21 paginiOccupational Profile and Intervention Plan Finalapi-263352281Încă nu există evaluări
- Running Head: Occupational Profile & Intervention Plan 1Document18 paginiRunning Head: Occupational Profile & Intervention Plan 1api-238107777Încă nu există evaluări
- New Intervention PlanDocument17 paginiNew Intervention Planapi-282753416Încă nu există evaluări
- Clients Goals To Address in SessionDocument8 paginiClients Goals To Address in Sessionapi-436429414Încă nu există evaluări
- Dickson Occupational ProfileDocument18 paginiDickson Occupational Profileapi-255001706Încă nu există evaluări
- Soap NoteDocument2 paginiSoap Noteapi-285542134Încă nu există evaluări
- Soap 11Document4 paginiSoap 11api-436429414Încă nu există evaluări
- Occupational Profile Intervention PlanDocument19 paginiOccupational Profile Intervention Planapi-263353704Încă nu există evaluări
- 630 Occupational Profile and Intervention PlanDocument22 pagini630 Occupational Profile and Intervention Planapi-282538590100% (1)
- Occupational Profile and Intervention PlanDocument18 paginiOccupational Profile and Intervention Planapi-282525755Încă nu există evaluări
- Eval Soap NoteDocument10 paginiEval Soap Noteapi-436577744Încă nu există evaluări
- Soap NoteDocument2 paginiSoap Noteapi-382628487Încă nu există evaluări
- Fieldwork Case Study Treatment Plan AssignmentDocument11 paginiFieldwork Case Study Treatment Plan Assignmentapi-398892840Încă nu există evaluări
- Model of Human Occupation Parts 1-4Document36 paginiModel of Human Occupation Parts 1-4Alice GiffordÎncă nu există evaluări
- Occupational Therapy Evaluation Report and Initial Intervention PlanDocument12 paginiOccupational Therapy Evaluation Report and Initial Intervention Planapi-488383880100% (1)
- Case Study Paper FinalDocument19 paginiCase Study Paper Finalapi-240832658Încă nu există evaluări
- Soap Note 2 Community ClientDocument12 paginiSoap Note 2 Community Clientapi-271984934Încă nu există evaluări
- Occupational Profile & Intervention PlanDocument19 paginiOccupational Profile & Intervention Planapi-262531856100% (1)
- Occupational Therapy in Obsesive Compulsive DisorderDocument3 paginiOccupational Therapy in Obsesive Compulsive DisorderManuela AlouÎncă nu există evaluări
- Occupations Profile & Intervention PlanDocument20 paginiOccupations Profile & Intervention Planapi-282223043Încă nu există evaluări
- Occupation Based InterventionsDocument16 paginiOccupation Based Interventionsapi-293182319100% (1)
- Stroke UE ToolkitDocument69 paginiStroke UE ToolkitWhitney JosephÎncă nu există evaluări
- Occupational Profile Intervention PlanDocument17 paginiOccupational Profile Intervention Planapi-264481356Încă nu există evaluări
- Occupational Profile Intervention Plan-Danielle PalmerDocument20 paginiOccupational Profile Intervention Plan-Danielle Palmerapi-292894327Încă nu există evaluări
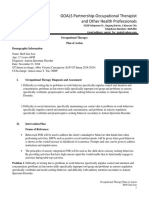
- GOALS Partnership-Occupational Therapist and Other Health ProfessionalsDocument5 paginiGOALS Partnership-Occupational Therapist and Other Health ProfessionalsarvinÎncă nu există evaluări
- Client Initial Evaluation Soap NoteDocument8 paginiClient Initial Evaluation Soap Noteapi-582889983Încă nu există evaluări
- Key Responsibilities:: Occupational Therapist Job Description V-Jan/2020Document4 paginiKey Responsibilities:: Occupational Therapist Job Description V-Jan/2020MD Luthfy LubisÎncă nu există evaluări
- Pediatric SpaDocument11 paginiPediatric Spaapi-420919156100% (2)
- Occupational Therapy Survival GuideDocument12 paginiOccupational Therapy Survival Guideapi-256686248Încă nu există evaluări
- Occupational Profile and Analysis Final EditedDocument14 paginiOccupational Profile and Analysis Final Editedapi-233645719Încă nu există evaluări
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Document54 pagini2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18Încă nu există evaluări
- Immuno Part CsDocument15 paginiImmuno Part CsCecilia TesoreroÎncă nu există evaluări
- Stroke Rehab Fact SheetDocument2 paginiStroke Rehab Fact SheetHendra PrayogaÎncă nu există evaluări
- Occupational Analysis Intervention PlanDocument19 paginiOccupational Analysis Intervention Planapi-293223028Încă nu există evaluări
- Meaningful OccupationDocument13 paginiMeaningful OccupationSyafiq Azzmi100% (1)
- 11 17 Soap NoteDocument4 pagini11 17 Soap Noteapi-435469413Încă nu există evaluări
- Occupational Therapy's Role in Diabetes Self ManagementDocument2 paginiOccupational Therapy's Role in Diabetes Self ManagementThe American Occupational Therapy AssociationÎncă nu există evaluări
- Soap NoteDocument1 paginăSoap Noteapi-519577267Încă nu există evaluări
- Occupational Therapy Toolbox Study GuideDocument44 paginiOccupational Therapy Toolbox Study GuideKristian ShumateÎncă nu există evaluări
- Stepping On CertificateDocument1 paginăStepping On Certificateapi-262531856Încă nu există evaluări
- Resume With No Contact Info PubDocument2 paginiResume With No Contact Info Pubapi-262531856Încă nu există evaluări
- Reflection On Social JusticeDocument2 paginiReflection On Social Justiceapi-262531856Încă nu există evaluări
- Research 504 Caffeine Consumption and Anxiety LevelsDocument11 paginiResearch 504 Caffeine Consumption and Anxiety Levelsapi-262531856Încă nu există evaluări
- Reflection On Occupation-Based PracticeDocument2 paginiReflection On Occupation-Based Practiceapi-262531856Încă nu există evaluări
- Leadership Development PlanDocument5 paginiLeadership Development Planapi-262531856Încă nu există evaluări
- Treating Baby B - A Jeune Syndrome Case StudyDocument21 paginiTreating Baby B - A Jeune Syndrome Case Studyapi-262531856Încă nu există evaluări
- Reflection On LeadershipDocument2 paginiReflection On Leadershipapi-262531856Încă nu există evaluări
- Addressing Cognition and Executive Function in Patients With Tbi & AbiDocument40 paginiAddressing Cognition and Executive Function in Patients With Tbi & Abiapi-262531856Încă nu există evaluări
- Goddard Occupational Analysis & Intervention PlanDocument23 paginiGoddard Occupational Analysis & Intervention Planapi-262531856Încă nu există evaluări
- Nevada Resources For Homeless ResidentsDocument2 paginiNevada Resources For Homeless Residentsapi-262531856Încă nu există evaluări
- Coordinated Intake Info Sheet Help Hope HomeDocument2 paginiCoordinated Intake Info Sheet Help Hope Homeapi-262531856Încă nu există evaluări
- Research Day-Nidcap - Goddard & Noss 2015Document16 paginiResearch Day-Nidcap - Goddard & Noss 2015api-262531856Încă nu există evaluări
- Reflection On Evidence-Based PracticeDocument2 paginiReflection On Evidence-Based Practiceapi-262531856Încă nu există evaluări
- HSH EvalDocument5 paginiHSH Evalapi-262531856Încă nu există evaluări
- Ncep EvalDocument4 paginiNcep Evalapi-262531856Încă nu există evaluări
- Opportunity Village EvalDocument5 paginiOpportunity Village Evalapi-262531856Încă nu există evaluări
- Sunrise Level II EvalDocument8 paginiSunrise Level II Evalapi-262531856Încă nu există evaluări
- Ccls CertificateDocument1 paginăCcls Certificateapi-262531856Încă nu există evaluări
- Pte PresidentDocument1 paginăPte Presidentapi-262531856Încă nu există evaluări
- Nidcap Poster Final Edited For Research DayDocument1 paginăNidcap Poster Final Edited For Research Dayapi-262531856Încă nu există evaluări
- Pi Theta InitiationDocument1 paginăPi Theta Initiationapi-262531856Încă nu există evaluări
- Cat Worksheet - Nidcap - Goddard & Noss FinalDocument11 paginiCat Worksheet - Nidcap - Goddard & Noss Finalapi-262531856Încă nu există evaluări
- Nota PresenterDocument1 paginăNota Presenterapi-262531856Încă nu există evaluări
- Addressing Cognition Poster 36x42Document1 paginăAddressing Cognition Poster 36x42api-262531856Încă nu există evaluări
- Evidence Paper On Adolescent Transitional ProgramsDocument14 paginiEvidence Paper On Adolescent Transitional Programsapi-262531856Încă nu există evaluări
- Activities For Book PDF VersionDocument12 paginiActivities For Book PDF Versionapi-262531856Încă nu există evaluări
- Cat Evidence Table - Nidcap - Goddard & Noss Final 1 in MarginsDocument28 paginiCat Evidence Table - Nidcap - Goddard & Noss Final 1 in Marginsapi-262531856Încă nu există evaluări
- Not Anymore Certificate of CompletionDocument1 paginăNot Anymore Certificate of Completionapi-262531856Încă nu există evaluări
- Home Assessment DocumentDocument8 paginiHome Assessment Documentapi-262531856Încă nu există evaluări
- From Solvay Magazine - 48 - Dec 2011 PDFDocument36 paginiFrom Solvay Magazine - 48 - Dec 2011 PDFchb2Încă nu există evaluări
- Commercial Arithmetics PDFDocument2 paginiCommercial Arithmetics PDFDawn50% (2)
- Architecture and Design Institute Project ReportDocument103 paginiArchitecture and Design Institute Project ReportAbi Kannan100% (1)
- Lee Pek Yi: by Authority of The Senate Be It Known ThatDocument4 paginiLee Pek Yi: by Authority of The Senate Be It Known Thatjoyslee96Încă nu există evaluări
- Srila Prabhupada On 64 Rounds - 0Document4 paginiSrila Prabhupada On 64 Rounds - 0Anton ArsenÎncă nu există evaluări
- Precalculus Honors ProjectDocument2 paginiPrecalculus Honors Projectapi-268267969Încă nu există evaluări
- BALMES Module1 Assingment Autobiography GECUTS 18Document3 paginiBALMES Module1 Assingment Autobiography GECUTS 18Loki DarwinÎncă nu există evaluări
- Are To Many People Going To CollegeDocument2 paginiAre To Many People Going To Collegektrout919Încă nu există evaluări
- MTO Drivers Handbook For Ontario, CanadaDocument145 paginiMTO Drivers Handbook For Ontario, CanadaJo PantulaÎncă nu există evaluări
- Lesson Plan Volleyball SettingDocument3 paginiLesson Plan Volleyball Settingapi-222021412Încă nu există evaluări
- Holy Child Catholic School v. Hon. Patricia Sto. TomasDocument10 paginiHoly Child Catholic School v. Hon. Patricia Sto. TomasEmir MendozaÎncă nu există evaluări
- Reaction Paper Tolentino John Carlo C.Document1 paginăReaction Paper Tolentino John Carlo C.john carlo tolentinoÎncă nu există evaluări
- Grade 6 Food Preservation Weekly LessonDocument67 paginiGrade 6 Food Preservation Weekly Lessonchona redillasÎncă nu există evaluări
- The What Why and How of Culturally Responsive Teaching International Mandates Challenges and OpportunitiesDocument18 paginiThe What Why and How of Culturally Responsive Teaching International Mandates Challenges and Opportunitiesapi-696560926Încă nu există evaluări
- School Safety Assessment Tool AnalysisDocument21 paginiSchool Safety Assessment Tool AnalysisRuel Gapuz ManzanoÎncă nu există evaluări
- Environmental Impact AssessmentDocument85 paginiEnvironmental Impact AssessmentAlexis Jabesa100% (1)
- Cambridge International General Certificate of Secondary EducationDocument20 paginiCambridge International General Certificate of Secondary Educationharshiththunkable31Încă nu există evaluări
- Thesis On Education System of PakistanDocument5 paginiThesis On Education System of Pakistaniouliakingbellevue100% (2)
- Broucher IiitdmjDocument34 paginiBroucher Iiitdmjapi-319983390Încă nu există evaluări
- 5E Lesson Plan Template: TeacherDocument6 pagini5E Lesson Plan Template: Teacherapi-515949514Încă nu există evaluări
- Effects of Peer Pressure on Academic Performance (40Document6 paginiEffects of Peer Pressure on Academic Performance (40MaynardMiranoÎncă nu există evaluări
- Iiit BhuvaneshwarDocument14 paginiIiit BhuvaneshwarsuburaajÎncă nu există evaluări
- Lords Institute of Engineering and TechnologyDocument4 paginiLords Institute of Engineering and TechnologyTAMMISETTY VIJAY KUMARÎncă nu există evaluări
- Koya University Faculty of Education: English DepartmentDocument7 paginiKoya University Faculty of Education: English Departmentnazaninmustafa647Încă nu există evaluări
- Pack Your Bags: Activity TypeDocument3 paginiPack Your Bags: Activity TypeBurak AkhanÎncă nu există evaluări
- MKTM028 2017 18 As1 MasterDocument9 paginiMKTM028 2017 18 As1 Masterprojectwork185Încă nu există evaluări
- Science Syllabus OverviewDocument1 paginăScience Syllabus Overviewapi-348858074Încă nu există evaluări
- Amanda Lesson PlanDocument7 paginiAmanda Lesson Planapi-2830820140% (1)
- CII Recognition: of Prior LearningDocument3 paginiCII Recognition: of Prior LearningShanmuganathan RamanathanÎncă nu există evaluări
- Report MastDocument512 paginiReport Mastrona thomasÎncă nu există evaluări