S-ar putea să vă placă și
- Systemic Lupus Erythematosus PathophysiologyDocument8 paginiSystemic Lupus Erythematosus PathophysiologySharmaineTaguitagOmli100% (1)
- Sle Concept Map Part 1Document1 paginăSle Concept Map Part 1Vane UcatÎncă nu există evaluări
- Pathophysiology of SLEDocument16 paginiPathophysiology of SLESeff CausapinÎncă nu există evaluări
- SLE Risk Factors and ComplicationsDocument5 paginiSLE Risk Factors and Complicationsjoyrena ochondraÎncă nu există evaluări
- Pa Tho Physiology Part 1Document1 paginăPa Tho Physiology Part 1anonymous89ify100% (2)
- SLE PathophysiologyDocument3 paginiSLE PathophysiologyRanela Kwinkee Pastor Salazar100% (7)
- SLE ANEMIA PATHOPHYSIOLOGYDocument1 paginăSLE ANEMIA PATHOPHYSIOLOGYGhan Maria100% (2)
- Pathophysiology of Rheumatoid ArthritisDocument1 paginăPathophysiology of Rheumatoid ArthritisGerardeanne ReposarÎncă nu există evaluări
- Case Study Systemic Lupus ErythematosusDocument54 paginiCase Study Systemic Lupus ErythematosusCharmaine Paran100% (3)
- Systemic Lupus Erythematosus (SLE) Is A Multiorgan System Autoimmune DiseaseDocument9 paginiSystemic Lupus Erythematosus (SLE) Is A Multiorgan System Autoimmune Diseasecoyre100% (2)
- SLE Concept MapDocument1 paginăSLE Concept Mapadrienne cervantesÎncă nu există evaluări
- Systemic Lupus ErythematosusDocument80 paginiSystemic Lupus ErythematosusLarissa Miguel Severa100% (2)
- PathoConceptMap AIDSDocument3 paginiPathoConceptMap AIDSKristen Babauta50% (2)
- Systemic Lupus Erythematosus PathophysiologyDocument8 paginiSystemic Lupus Erythematosus PathophysiologyAnonymous OU6w8lX9Încă nu există evaluări
- Lupus, SLEDocument2 paginiLupus, SLEFrances Anne Pasiliao100% (2)
- Guide to Systemic Lupus Erythematosus (SLE): Causes, Symptoms, Diagnosis & TreatmentDocument25 paginiGuide to Systemic Lupus Erythematosus (SLE): Causes, Symptoms, Diagnosis & TreatmentdaliaÎncă nu există evaluări
- Systemic Lupous Erythematosus (SLE)Document46 paginiSystemic Lupous Erythematosus (SLE)Power La Victoria Floro100% (1)
- Systemic Lupus ErythematosusDocument13 paginiSystemic Lupus ErythematosusGrace RoselinyÎncă nu există evaluări
- Dengue PoathoDocument6 paginiDengue PoathoCleobebs Agustin100% (1)
- ALL PathophysiologyDocument2 paginiALL PathophysiologyDeo Michael Rivera LlamasÎncă nu există evaluări
- Dengue Hemorrhagic Fever Pathophysiology DiagramDocument4 paginiDengue Hemorrhagic Fever Pathophysiology DiagramCyrus De Asis67% (3)
- Leukemia With PathophysiologyDocument34 paginiLeukemia With Pathophysiologymabec pagaduan90% (41)
- Pathophysiology - Rheumatoid ArthritisDocument1 paginăPathophysiology - Rheumatoid ArthritisAngel FiloteoÎncă nu există evaluări
- Pathophysiology of Breast Cancer: Predisposing Factors, Cell Changes, SymptomsDocument1 paginăPathophysiology of Breast Cancer: Predisposing Factors, Cell Changes, SymptomsEggy Pascual100% (1)
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 paginiPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Pathophysiology of TuberculosisDocument3 paginiPathophysiology of TuberculosisMonica Marie Morales86% (14)
- Pathophysiology AML DiagramDocument4 paginiPathophysiology AML DiagramKlerra Hope60% (5)
- HIV Simple Case StudyDocument13 paginiHIV Simple Case StudyJanna Pimentel100% (1)
- Pathophysiology of Hepatitis B Virus InfectionDocument9 paginiPathophysiology of Hepatitis B Virus InfectionDianne G Ignacio100% (4)
- Systemic Lupus ErythematosusDocument9 paginiSystemic Lupus ErythematosusTheeya QuigaoÎncă nu există evaluări
- 1.pathophysiology of MeningitisDocument1 pagină1.pathophysiology of Meningitisshielamaygo05100% (1)
- Systemic Lupus ErythematosusDocument64 paginiSystemic Lupus Erythematosusganga2424100% (1)
- Acute Lymphoblastic Leukemia Pathophysiology SummaryDocument3 paginiAcute Lymphoblastic Leukemia Pathophysiology SummarymonishaÎncă nu există evaluări
- Dengue Hemorrhagic Fever PathophysiologyDocument4 paginiDengue Hemorrhagic Fever Pathophysiologyteddydeclines1483% (18)
- Pathophysiology of Nephrotic SyndromeDocument1 paginăPathophysiology of Nephrotic SyndromeRan MaÎncă nu există evaluări
- Acute Lymphocytic Leukemia FinalDocument30 paginiAcute Lymphocytic Leukemia FinalYuwi50% (2)
- NCP Nursing Care Plans For Aplastic AnemiaDocument3 paginiNCP Nursing Care Plans For Aplastic AnemiaTahir Ali0% (1)
- Systemic Lupus ErythematosusDocument2 paginiSystemic Lupus ErythematosusErnest caneteÎncă nu există evaluări
- Pathophysiology - Diabetes Mellitus Type 2Document3 paginiPathophysiology - Diabetes Mellitus Type 2Francis Kevin Sagudo100% (10)
- Lupus Case ReportDocument1 paginăLupus Case ReportMendy HararyÎncă nu există evaluări
- Pathophysiology of StrokeDocument3 paginiPathophysiology of StrokeAqeel Al-Mahdaly0% (1)
- Systemic Lupus ErythematosusDocument31 paginiSystemic Lupus ErythematosusJerilee SoCute WattsÎncă nu există evaluări
- Diabetes Mellitus Type 2 Schematic DiagramDocument1 paginăDiabetes Mellitus Type 2 Schematic DiagramJhe Lyn82% (11)
- Pa Tho Physiology of Meningioma (Edited Version)Document2 paginiPa Tho Physiology of Meningioma (Edited Version)Niño Villamarin71% (7)
- Pathophysiology Dengue Hemorrhagic FeverDocument1 paginăPathophysiology Dengue Hemorrhagic Fevershiramu33% (3)
- Myesthenia GravisDocument3 paginiMyesthenia GravisJorie RocoÎncă nu există evaluări
- LupusDocument28 paginiLupusRiin IrasustaÎncă nu există evaluări
- SLE Patogenesis & Patofisiologi PDFDocument8 paginiSLE Patogenesis & Patofisiologi PDFRIZQI IRFANSYAH100% (1)
- Systemic Lupus Erythematosus (SLE) Pathogenesis and ManifestationsDocument10 paginiSystemic Lupus Erythematosus (SLE) Pathogenesis and Manifestationsinah krizia lagueÎncă nu există evaluări
- Pa Tho Physiology Sle, CompDocument5 paginiPa Tho Physiology Sle, CompHassan Bj MarabongÎncă nu există evaluări
- Valmed PathoDocument1 paginăValmed PathoJez RarangÎncă nu există evaluări
- Med 1.11 - SleDocument5 paginiMed 1.11 - SleZazaÎncă nu există evaluări
- ImunitasDocument7 paginiImunitasdeeÎncă nu există evaluări
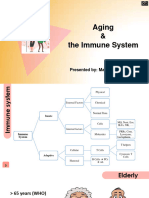
- 7-Aging and The Immune System - DR - TaghaviDocument42 pagini7-Aging and The Immune System - DR - TaghavihumairashowkatÎncă nu există evaluări
- Autoimmunity GuideDocument5 paginiAutoimmunity GuideJoshua Ty CayetanoÎncă nu există evaluări
- Pertaining To Extracellular Fluid Such As Plasma and Lymph. The Term Humoral Immunity Is Used To Denote Antibody Mediated Immune ResponsesDocument4 paginiPertaining To Extracellular Fluid Such As Plasma and Lymph. The Term Humoral Immunity Is Used To Denote Antibody Mediated Immune ResponsesZhon CabitacÎncă nu există evaluări
- Imun AwalDocument13 paginiImun AwalAdy RAstafaraÎncă nu există evaluări
- SCIDDocument9 paginiSCIDgarimaupadhyay20002Încă nu există evaluări
- Immune Regulation and ToleranceDocument33 paginiImmune Regulation and ToleranceAniruddha RoyÎncă nu există evaluări
- Chapter 50 Assessment of Immune FunctionDocument12 paginiChapter 50 Assessment of Immune FunctionChan SorianoÎncă nu există evaluări
- The Three Musketeers by Alexandre DumasDocument729 paginiThe Three Musketeers by Alexandre DumasBooks100% (5)
- Abruptio Placenta PathophysiologyDocument4 paginiAbruptio Placenta Pathophysiologyjamie carpioÎncă nu există evaluări
- HR Report FinalDocument16 paginiHR Report FinalkathyÎncă nu există evaluări
- ARF PathophysiologyDocument2 paginiARF Pathophysiologykathy100% (9)
- DIC PathophysiologyDocument1 paginăDIC Pathophysiologykathy100% (1)
- Placenta Previa PathophysiologyDocument1 paginăPlacenta Previa Pathophysiologykathy85% (20)
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Liver CirrhosisDocument76 paginiLiver Cirrhosiskathy100% (2)
- Guillain Barre Syndrome PathophysiologyDocument4 paginiGuillain Barre Syndrome Pathophysiologykathy100% (13)
- Substance DependenceDocument157 paginiSubstance DependencekathyÎncă nu există evaluări
- CP On OsteomyelitisDocument147 paginiCP On Osteomyelitiskathy50% (2)
- CHNDocument59 paginiCHNkathy100% (1)
- THESIS in NURSINGDocument47 paginiTHESIS in NURSINGkathy85% (40)
- ER PowerpointDocument144 paginiER Powerpointkathy100% (1)
- CP-Guillain Barre SyndromeDocument35 paginiCP-Guillain Barre Syndromekathy60% (5)
- CP On Breast CancerDocument100 paginiCP On Breast Cancerkathy50% (2)
- CP Placenta PreviaDocument95 paginiCP Placenta Previakathy60% (5)
- CP On Pre-EclampsiaDocument152 paginiCP On Pre-Eclampsiakathy100% (2)
- CVADocument116 paginiCVAkathy100% (1)
- CP On Calculous CholelithiasisDocument102 paginiCP On Calculous Cholelithiasiskathy100% (3)
- CP On AmoebiasisDocument77 paginiCP On Amoebiasiskathy100% (1)
- Overweight and Obesity in AmericaDocument10 paginiOverweight and Obesity in Americamzvette234Încă nu există evaluări
- Mathematical Language and Symbols ExplainedDocument5 paginiMathematical Language and Symbols Explainedcyra6flores6verderaÎncă nu există evaluări
- Bailable and Non BailableDocument10 paginiBailable and Non BailableasthaÎncă nu există evaluări
- Edith Bonomi CV SummaryDocument1 paginăEdith Bonomi CV SummaryEdithÎncă nu există evaluări
- Advocacy Plan Final Edec 435Document11 paginiAdvocacy Plan Final Edec 435api-375034422Încă nu există evaluări
- ''Let All God's Angels Worship Him'' - Gordon AllanDocument8 pagini''Let All God's Angels Worship Him'' - Gordon AllanRubem_CLÎncă nu există evaluări
- Number System ConversionDocument26 paginiNumber System ConversionMahesh Chandra UpadhyayÎncă nu există evaluări
- SAP FICO Asset Accounting 1Document3 paginiSAP FICO Asset Accounting 1Ananthakumar AÎncă nu există evaluări
- QuitclaimDocument2 paginiQuitclaimAlfred Hernandez CampañanoÎncă nu există evaluări
- 15 Tips To Get Fair Skin Naturally PDFDocument2 pagini15 Tips To Get Fair Skin Naturally PDFLatha SivakumarÎncă nu există evaluări
- ARGUMENTS AGAINST AND IN FAVOR OF THE DEATH PENALTYDocument18 paginiARGUMENTS AGAINST AND IN FAVOR OF THE DEATH PENALTYRod Herrero PinoÎncă nu există evaluări
- Initial Evaluation in The 11th Form B1 LevelDocument2 paginiInitial Evaluation in The 11th Form B1 LevelDumitru GruscaÎncă nu există evaluări
- Philippians 1:27-2:18Document3 paginiPhilippians 1:27-2:18Buddy OvermanÎncă nu există evaluări
- RitesDocument11 paginiRitesMadmen quillÎncă nu există evaluări
- Female by CourseDocument40 paginiFemale by CourseMohamed AymanÎncă nu există evaluări
- 6710 NotesDocument45 pagini6710 NotesAndrés SuquilloÎncă nu există evaluări
- GUINNESS F13 Full Year BriefingDocument27 paginiGUINNESS F13 Full Year BriefingImoUstino ImoÎncă nu există evaluări
- Brochure KTM April 2008Document2 paginiBrochure KTM April 2008sthapitÎncă nu există evaluări
- Parle Sales DistributionDocument21 paginiParle Sales Distributionkakki1088Încă nu există evaluări
- Princes of the Apocalypse Locations IndexDocument2 paginiPrinces of the Apocalypse Locations IndexPedroManzelaDuarteÎncă nu există evaluări
- Copyright Protection for TV Show FormatsDocument11 paginiCopyright Protection for TV Show FormatsJoy Navaja DominguezÎncă nu există evaluări
- Ziarat e NahiyaDocument48 paginiZiarat e Nahiyazaighama_1100% (7)
- Physics 5th Edition Walker Test BankDocument24 paginiPhysics 5th Edition Walker Test BankKathyHernandeznobt100% (31)
- Kamala Das Poetry CollectionDocument0 paginiKamala Das Poetry CollectionBasa SwaminathanÎncă nu există evaluări
- Memorial On Behalf of PetitionerDocument35 paginiMemorial On Behalf of PetitionerAjitabhGoel67% (3)
- LIC Jeevan Labh Plan (836) DetailsDocument12 paginiLIC Jeevan Labh Plan (836) DetailsMuthukrishnan SankaranÎncă nu există evaluări
- Research Scholar Progress Report Review FormDocument3 paginiResearch Scholar Progress Report Review FormYepuru ChaithanyaÎncă nu există evaluări
- Adler Individual-PsychologyDocument3 paginiAdler Individual-PsychologyPORRAS, REJEAN ANN D.Încă nu există evaluări
- Chong Co Thai Restaurant LocationsDocument19 paginiChong Co Thai Restaurant LocationsrajragavendraÎncă nu există evaluări