S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Pharmacy Risk Management PlanDocument6 paginiPharmacy Risk Management PlanJohn Roa75% (8)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Letter To The President of Indonesia COVID-19 and Tobacco Smoking-Call To Action by 42 Prominent Organizations English Version April 15, 2020Document6 paginiLetter To The President of Indonesia COVID-19 and Tobacco Smoking-Call To Action by 42 Prominent Organizations English Version April 15, 2020bobbyramakant100% (1)
- Presentation of Audrey M Battu From Clinton Health Access Initiative (CHAI)Document17 paginiPresentation of Audrey M Battu From Clinton Health Access Initiative (CHAI)bobbyramakant0% (1)
- Collaboration Issues and Models - Within and Outside Nursing)Document14 paginiCollaboration Issues and Models - Within and Outside Nursing)madhurima kundu44% (9)
- Australia and Taiwan's Memorandum of Understanding - Medical TransfersDocument12 paginiAustralia and Taiwan's Memorandum of Understanding - Medical TransfersBuzzFeedOz100% (1)
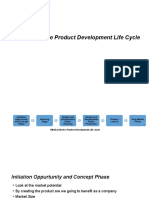
- Medical Device Product Development Life CycleDocument8 paginiMedical Device Product Development Life CycleSuresh Anand100% (1)
- The Cost of "Growing Up"Document15 paginiThe Cost of "Growing Up"bobbyramakantÎncă nu există evaluări
- Access To Male Family Planning Methods in Timor-Leste - Preliminary Findings From A Qualitative Participatory Research ProjectDocument14 paginiAccess To Male Family Planning Methods in Timor-Leste - Preliminary Findings From A Qualitative Participatory Research ProjectbobbyramakantÎncă nu există evaluări
- Abstract Presentation: Anna Ravendran and Kate Burry of Family Planning New Zealand (SRHR in Rural Vanuatu: Knowledge, Access and Barriers)Document14 paginiAbstract Presentation: Anna Ravendran and Kate Burry of Family Planning New Zealand (SRHR in Rural Vanuatu: Knowledge, Access and Barriers)bobbyramakantÎncă nu există evaluări
- Leveraging Sport To Improve Perceptions of Violence and Sexual and Reproductive Health and Rights For AdolescentsDocument12 paginiLeveraging Sport To Improve Perceptions of Violence and Sexual and Reproductive Health and Rights For AdolescentsbobbyramakantÎncă nu există evaluări
- Plenary Presentation: Karen Hill (SRHR in The Pacific: Strategic Approach)Document18 paginiPlenary Presentation: Karen Hill (SRHR in The Pacific: Strategic Approach)bobbyramakantÎncă nu există evaluări
- Opportunities For Strengthening Sexual Health Education in SchoolsDocument13 paginiOpportunities For Strengthening Sexual Health Education in SchoolsbobbyramakantÎncă nu există evaluări
- DR Gilada - Intervention Application Before Hon. SCI - FinalDocument18 paginiDR Gilada - Intervention Application Before Hon. SCI - FinalbobbyramakantÎncă nu există evaluări
- The Leader Lies in You (Success Stories of Women Farmers in UP, India)Document68 paginiThe Leader Lies in You (Success Stories of Women Farmers in UP, India)bobbyramakantÎncă nu există evaluări
- Health Experts Meet Telangana Governor DR Tamilisai Soundararajan: Memorandum Submitted To Telangana GovernorDocument2 paginiHealth Experts Meet Telangana Governor DR Tamilisai Soundararajan: Memorandum Submitted To Telangana GovernorbobbyramakantÎncă nu există evaluări
- Shreya Rawal and Durgesh Nandan Yadav Poster On SolidarityDocument1 paginăShreya Rawal and Durgesh Nandan Yadav Poster On SolidaritybobbyramakantÎncă nu există evaluări
- Presentation of Anne Jones OAM in Lead Up To World Cancer Day 2017Document12 paginiPresentation of Anne Jones OAM in Lead Up To World Cancer Day 2017bobbyramakantÎncă nu există evaluări
- Needs of Comprehensive Sexuality Education (Cse) of Students in Thai Nguyen University (Tnu), VietnamDocument15 paginiNeeds of Comprehensive Sexuality Education (Cse) of Students in Thai Nguyen University (Tnu), VietnambobbyramakantÎncă nu există evaluări
- Presentation of DR Archana Trivedi, One of Co-Authors of Study On Mhealth and TBDocument11 paginiPresentation of DR Archana Trivedi, One of Co-Authors of Study On Mhealth and TBbobbyramakantÎncă nu există evaluări
- DR Shivani Sharma Pandey's Slides On Challenges With Autistic ChildrenDocument6 paginiDR Shivani Sharma Pandey's Slides On Challenges With Autistic ChildrenbobbyramakantÎncă nu există evaluări
- Webinar Presentation of Cristina Parsons Perez of NCD AllianceDocument12 paginiWebinar Presentation of Cristina Parsons Perez of NCD AlliancebobbyramakantÎncă nu există evaluări
- Presentation of DR Rita Banik, Founder President of 'RACE To Rein in Cancer'Document18 paginiPresentation of DR Rita Banik, Founder President of 'RACE To Rein in Cancer'bobbyramakantÎncă nu există evaluări
- Dean PresentationDocument33 paginiDean PresentationbobbyramakantÎncă nu există evaluări
- DR Nguyen Viet Nhung's Presentation in #endTB WebinarDocument10 paginiDR Nguyen Viet Nhung's Presentation in #endTB WebinarbobbyramakantÎncă nu există evaluări
- Report On Inter-Sectoral Meeting On Youth's SRHRDocument22 paginiReport On Inter-Sectoral Meeting On Youth's SRHRbobbyramakantÎncă nu există evaluări
- Webinar Presentations of Prof Anand Mishra and DR Pooja Ramakant From Endocrine Surgery Dept of KGMUDocument35 paginiWebinar Presentations of Prof Anand Mishra and DR Pooja Ramakant From Endocrine Surgery Dept of KGMUbobbyramakantÎncă nu există evaluări
- World No Tobacco Day 2017 Webinar Presentation of Michelle Syonne Reyes-PalmonesDocument20 paginiWorld No Tobacco Day 2017 Webinar Presentation of Michelle Syonne Reyes-PalmonesbobbyramakantÎncă nu există evaluări
- Presentation of DR Ajay Mishra of Nelson Hospital, IndiaDocument6 paginiPresentation of DR Ajay Mishra of Nelson Hospital, IndiabobbyramakantÎncă nu există evaluări
- Acid& Chemical Burns Part ADocument10 paginiAcid& Chemical Burns Part ASojiÎncă nu există evaluări
- COVID-19 Response - Living With COVID-19Document63 paginiCOVID-19 Response - Living With COVID-19eman mamdohÎncă nu există evaluări
- Anatomi Berorientasi Klinis: A. Sentot Suropati. Dr. SPPD, FinasimDocument47 paginiAnatomi Berorientasi Klinis: A. Sentot Suropati. Dr. SPPD, FinasimYudhistira NugrahaÎncă nu există evaluări
- Recognized Nursing Colleges in Tamil NaduDocument31 paginiRecognized Nursing Colleges in Tamil Naduprasadden100% (1)
- DNB CetssDocument21 paginiDNB CetssRinku RinkuÎncă nu există evaluări
- Health Care Access Dental Clinic ProvidersDocument31 paginiHealth Care Access Dental Clinic ProvidersJake MendozaÎncă nu există evaluări
- New Resume 2018Document3 paginiNew Resume 2018api-400660952Încă nu există evaluări
- Clinical Skill - Advance History TakingDocument20 paginiClinical Skill - Advance History TakingJason CalvinÎncă nu există evaluări
- This Study Resource WasDocument2 paginiThis Study Resource WasAbhishek SachdevaÎncă nu există evaluări
- Urinary Retention PostpartumDocument5 paginiUrinary Retention PostpartumpaswordnyalupaÎncă nu există evaluări
- Jacinto CovitDocument4 paginiJacinto CovitJohanna AldanaÎncă nu există evaluări
- RRL and RRSDocument6 paginiRRL and RRSJAY LORRAINE PALACATÎncă nu există evaluări
- Medical Termination of Pregnancy Act, 1971Document4 paginiMedical Termination of Pregnancy Act, 1971Manjeet SinghÎncă nu există evaluări
- DIR-FLoortime Interested Providers 020311Document2 paginiDIR-FLoortime Interested Providers 020311circlestretchÎncă nu există evaluări
- CPG Philippine Clinical Practice Guideline On Palliative and End of Life Care For Adults With CancerDocument225 paginiCPG Philippine Clinical Practice Guideline On Palliative and End of Life Care For Adults With CancermjartezaÎncă nu există evaluări
- Fundamentals of Nursing 1St Edition Yoost Test Bank Full Chapter PDFDocument32 paginiFundamentals of Nursing 1St Edition Yoost Test Bank Full Chapter PDFSaraSmithczqs100% (12)
- Nurs FPX 4010 Assessment 3 Interdisciplinary Plan ProposalDocument5 paginiNurs FPX 4010 Assessment 3 Interdisciplinary Plan Proposalfarwaamjad771Încă nu există evaluări
- Family Nursing Care Plan-ChnDocument3 paginiFamily Nursing Care Plan-ChnChristine SaliganÎncă nu există evaluări
- Ethical Decision MakingDocument5 paginiEthical Decision Makingapi-491453387Încă nu există evaluări
- 3.23.2021 Vaccine Report Lifespan CNEDocument8 pagini3.23.2021 Vaccine Report Lifespan CNEFrank MaradiagaÎncă nu există evaluări
- B2B Assignment OnDocument20 paginiB2B Assignment OnRaju Kumar SharmaÎncă nu există evaluări
- RumenotomyDocument1 paginăRumenotomymake it make senseÎncă nu există evaluări
- WHO 2019 nCoV Therapeutics 2022.5 EngDocument141 paginiWHO 2019 nCoV Therapeutics 2022.5 EngBinish KansaraÎncă nu există evaluări
- Cut and Paste Types of Housing and DesignDocument2 paginiCut and Paste Types of Housing and Designapi-509516948Încă nu există evaluări
- Review of Related LiteratureDocument15 paginiReview of Related LiteratureGellie BuenaventuraÎncă nu există evaluări
- E000367 FullDocument15 paginiE000367 FullBBD BBDÎncă nu există evaluări