S-ar putea să vă placă și
- An Activity-Based Approach To Early Intervention by Joann Johnson Naomi Rahn Diane BrickerDocument424 paginiAn Activity-Based Approach To Early Intervention by Joann Johnson Naomi Rahn Diane BrickerPrecious Anne CastilloÎncă nu există evaluări
- (Insert Learn More About Margin Note 14.1 Here) : Pierangelo CH 14-1Document22 pagini(Insert Learn More About Margin Note 14.1 Here) : Pierangelo CH 14-1prakashborade6Încă nu există evaluări
- Jennings Informal Reading AssessmentDocument53 paginiJennings Informal Reading AssessmentJoy Ledesma Fabros Domingo100% (2)
- Zones of Regulation Vs Mind UpDocument43 paginiZones of Regulation Vs Mind Upapi-290229666Încă nu există evaluări
- Teacher Resource: Summary of SIOP Model ComponentsDocument1 paginăTeacher Resource: Summary of SIOP Model Componentsjmercier74Încă nu există evaluări
- Blake Garcia Iep Case StudyDocument16 paginiBlake Garcia Iep Case Studyapi-297423331Încă nu există evaluări
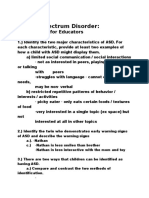
- Outline: Autism Spectrum Disorder (Part 1)Document8 paginiOutline: Autism Spectrum Disorder (Part 1)Reese MÎncă nu există evaluări
- Class Wide Behavior Management PlanDocument33 paginiClass Wide Behavior Management PlanGaby MontesÎncă nu există evaluări
- Nina M. Kurfman: 927 Village Park Way Savoy, IL 61874 (309) 531-3669Document3 paginiNina M. Kurfman: 927 Village Park Way Savoy, IL 61874 (309) 531-3669njohnso8Încă nu există evaluări
- Twice Exceptional HandoutDocument2 paginiTwice Exceptional Handoutapi-301904910Încă nu există evaluări
- U.S. History Regents Study GuideDocument16 paginiU.S. History Regents Study GuideSam_Buchbinder_8615Încă nu există evaluări
- Screening For Social Emotional Concerns: Considerations in The Selection of Instruments January 2009Document18 paginiScreening For Social Emotional Concerns: Considerations in The Selection of Instruments January 2009healthoregon100% (1)
- Lesson Plan and Instructional Program Format Moderate Lesson PlanDocument4 paginiLesson Plan and Instructional Program Format Moderate Lesson Planapi-251649080Încă nu există evaluări
- Empowering Parents & Teachers: How Parents and Teachers Can Develop Collaborative PartnershipsDe la EverandEmpowering Parents & Teachers: How Parents and Teachers Can Develop Collaborative PartnershipsÎncă nu există evaluări
- Dir - Floortime Model - Using Relationship-Based Intervention To IncDocument33 paginiDir - Floortime Model - Using Relationship-Based Intervention To IncAndreia SilvaÎncă nu există evaluări
- Manual For The Motor Imitation Scale (MIS) : Revised August 2015Document7 paginiManual For The Motor Imitation Scale (MIS) : Revised August 2015Kaaynat KhanÎncă nu există evaluări
- 3 ReinforcementDocument18 pagini3 ReinforcementZainab JamilÎncă nu există evaluări
- Self MonitoringDocument9 paginiSelf MonitoringNgọc TrầnÎncă nu există evaluări
- Autism: A Practical Guide for ParentsDe la EverandAutism: A Practical Guide for ParentsÎncă nu există evaluări
- Engleza Bilingv - Subiectul II - Variante 001-100 - An 2008Document155 paginiEngleza Bilingv - Subiectul II - Variante 001-100 - An 2008Admin75% (4)
- School-Based Interventions For AdhdDocument19 paginiSchool-Based Interventions For Adhdapi-290229666Încă nu există evaluări
- Classroom Group Sensory Experiences: Teachers Resource Series, #3De la EverandClassroom Group Sensory Experiences: Teachers Resource Series, #3Încă nu există evaluări
- Working With Asperger in The Classroom PDFDocument177 paginiWorking With Asperger in The Classroom PDFMahmoud AlFarajÎncă nu există evaluări
- DyslexiaDocument15 paginiDyslexiaapi-241268840Încă nu există evaluări
- Arts and Crafts of Davao and Zamboanga CityDocument26 paginiArts and Crafts of Davao and Zamboanga CityCarmi C. Paciente0% (1)
- WestbyDocument3 paginiWestbySwathi GÎncă nu există evaluări
- Speech & Language Therapy in Practice, Spring 2009Document32 paginiSpeech & Language Therapy in Practice, Spring 2009Speech & Language Therapy in PracticeÎncă nu există evaluări
- Editorial: Early Prevention and Intervention - The Five W (And One H) QuestionsDocument3 paginiEditorial: Early Prevention and Intervention - The Five W (And One H) QuestionsArwenÎncă nu există evaluări
- GREER & KEOHANE - The Evolution of Verbal Behavior in Children - The Journal of Speech-Language Pathology and Applied Behavior Analysis PDFDocument30 paginiGREER & KEOHANE - The Evolution of Verbal Behavior in Children - The Journal of Speech-Language Pathology and Applied Behavior Analysis PDFWilly Bosch100% (1)
- Supporting Social Competence in Children Who Use AacDocument9 paginiSupporting Social Competence in Children Who Use Aacapi-249986210100% (1)
- Classroom Accommodations Students AdhdDocument1 paginăClassroom Accommodations Students AdhdMeagan JonesÎncă nu există evaluări
- ASD Education ResourcesDocument4 paginiASD Education ResourcestracycwÎncă nu există evaluări
- (2017) Empowering Preschool Teachers To Identify Mental Health Problems A Task-Sharing Intervention in EthiopiaDocument11 pagini(2017) Empowering Preschool Teachers To Identify Mental Health Problems A Task-Sharing Intervention in EthiopiaJulián A. RamírezÎncă nu există evaluări
- Efficacy of An Early Intervention Program For At-Risk Preschool Boys: A Two-Group Control StudyDocument9 paginiEfficacy of An Early Intervention Program For At-Risk Preschool Boys: A Two-Group Control StudyMarina EÎncă nu există evaluări
- Child StudyDocument29 paginiChild Studyapi-501003650Încă nu există evaluări
- The Legacy of Early Humans To Contemporary Population 1Document35 paginiThe Legacy of Early Humans To Contemporary Population 1Norberto Ramirez Furto Jr.78% (9)
- Dynamic Assessment of Young ChildrenDocument51 paginiDynamic Assessment of Young ChildrenreggelkeÎncă nu există evaluări
- Assistive Technology in Special Education and The Design For LearningDocument6 paginiAssistive Technology in Special Education and The Design For LearningJULIANA SANTOS MONTEIRO VIEIRAÎncă nu există evaluări
- Inclusive Practices 2 PDFDocument43 paginiInclusive Practices 2 PDFMarlene D VieiraÎncă nu există evaluări
- Special Needs and Inclusive Education: Doctoral thesisDe la EverandSpecial Needs and Inclusive Education: Doctoral thesisEvaluare: 5 din 5 stele5/5 (1)
- Effective Strategies For General and Special Education TeachersDocument72 paginiEffective Strategies For General and Special Education TeacherssasterahatikuÎncă nu există evaluări
- IRIS - AutismDocument7 paginiIRIS - Autismrianna Learn100% (1)
- Early Intervention Preschool Research/Process WorkDocument43 paginiEarly Intervention Preschool Research/Process WorkMurphy C0% (1)
- Aided Language Modeling SummaryDocument1 paginăAided Language Modeling Summaryapi-467320718Încă nu există evaluări
- Infant or Toddler Language Development Observation 1Document6 paginiInfant or Toddler Language Development Observation 1api-483246034Încă nu există evaluări
- Lisa Mcguire Final Research Project Week 5Document11 paginiLisa Mcguire Final Research Project Week 5Lisa McGuireÎncă nu există evaluări
- Personal and Professional IdentityDocument6 paginiPersonal and Professional Identityapi-584626247Încă nu există evaluări
- Developmental Milestone Analysis ProjectDocument12 paginiDevelopmental Milestone Analysis Projectapi-402669825Încă nu există evaluări
- RejectedDocument2 paginiRejectedAutismeyeÎncă nu există evaluări
- Peer Modeling AsdDocument20 paginiPeer Modeling Asdapi-320185546Încă nu există evaluări
- Tally Event SamplingDocument7 paginiTally Event Samplingapi-237394235Încă nu există evaluări
- Zone of Proximal DevelopmentDocument15 paginiZone of Proximal Developmentapi-280857978Încă nu există evaluări
- Overview of Aspergers SyndromeDocument2 paginiOverview of Aspergers Syndromeapi-237515534100% (1)
- Inclusion and Placement Decisions For Students With Special NeedsDocument11 paginiInclusion and Placement Decisions For Students With Special NeedsDaYs DaysÎncă nu există evaluări
- Shapiro - Cognitive FlexibilityDocument20 paginiShapiro - Cognitive FlexibilityDavid HallÎncă nu există evaluări
- Assignment1 ECL310 NaomiMathew 212198847Document20 paginiAssignment1 ECL310 NaomiMathew 212198847Naomi MathewÎncă nu există evaluări
- Autism - Literature ReviewDocument10 paginiAutism - Literature Reviewapi-446507356Încă nu există evaluări
- Circle of FriendsDocument3 paginiCircle of FriendsAldo Javier BarberoÎncă nu există evaluări
- Baierl Task Analysis and Chaining ProjectDocument15 paginiBaierl Task Analysis and Chaining Projectapi-354321926Încă nu există evaluări
- Text Complexity AppleDocument2 paginiText Complexity Appleapi-350961453Încă nu există evaluări
- Measuring Behavior Case StudyDocument31 paginiMeasuring Behavior Case Studyapi-265973793100% (1)
- What Are The Characteristics of A Teacher Who Can Established A WellDocument6 paginiWhat Are The Characteristics of A Teacher Who Can Established A WellVhiy Dizon BantingÎncă nu există evaluări
- Pbis IntroDocument49 paginiPbis Introapi-453886002Încă nu există evaluări
- Kernel Essays: Reviving The Essay Gretchen Bernabei How To Teach Structure Without FormulaDocument17 paginiKernel Essays: Reviving The Essay Gretchen Bernabei How To Teach Structure Without Formulahicham96Încă nu există evaluări
- Creativity in Preschool AssessmentDocument15 paginiCreativity in Preschool AssessmentEstera Daniela GavrilutÎncă nu există evaluări
- About Me: Amy DonovanDocument1 paginăAbout Me: Amy Donovanapi-290229666Încă nu există evaluări
- Quiz 2Document4 paginiQuiz 2api-290229666Încă nu există evaluări
- Request For Assessment Form: Situation Problem Behavior Most Common ResultDocument10 paginiRequest For Assessment Form: Situation Problem Behavior Most Common Resultapi-290229666Încă nu există evaluări
- Running Head: Response To Intervention: A Critical ReviewDocument11 paginiRunning Head: Response To Intervention: A Critical Reviewapi-290229666Încă nu există evaluări
- Odd PresentationDocument47 paginiOdd Presentationapi-290229666Încă nu există evaluări
- Ethics-Creation of Mock Counselling CentreDocument22 paginiEthics-Creation of Mock Counselling Centreapi-290229666Încă nu există evaluări
- Interventions For Self-Regulation - A Lit ReviewDocument12 paginiInterventions For Self-Regulation - A Lit Reviewapi-290229666Încă nu există evaluări
- Journal Entry - Prereferral InterventionDocument4 paginiJournal Entry - Prereferral Interventionapi-290229666Încă nu există evaluări
- Ethics-Creation of Mock Counselling CentreDocument22 paginiEthics-Creation of Mock Counselling Centreapi-290229666Încă nu există evaluări
- Nasp ReflectionDocument4 paginiNasp Reflectionapi-290229666Încă nu există evaluări
- Case Presentation May 2015Document20 paginiCase Presentation May 2015api-290229666Încă nu există evaluări
- History of AnxietyDocument15 paginiHistory of Anxietyapi-290229666Încă nu există evaluări
- Mock Research Proposal AssignmentDocument3 paginiMock Research Proposal Assignmentapi-290229666Încă nu există evaluări
- Research Article CritiqueDocument9 paginiResearch Article Critiqueapi-290229666Încă nu există evaluări
- Paper Reading FluencyDocument14 paginiPaper Reading Fluencyapi-290229666Încă nu există evaluări
- EDPS 612.03 Learning Task 2 Debate Analysis Paper: Amy DonovanDocument6 paginiEDPS 612.03 Learning Task 2 Debate Analysis Paper: Amy Donovanapi-290229666Încă nu există evaluări
- Ethics Paper-Final DraftDocument19 paginiEthics Paper-Final Draftapi-290229666Încă nu există evaluări
- GenogrampublisherDocument2 paginiGenogrampublisherapi-290229666Încă nu există evaluări
- Assessment Framework HandoutDocument3 paginiAssessment Framework Handoutapi-290229666Încă nu există evaluări
- Role of Parenting in Self-RegDocument10 paginiRole of Parenting in Self-Regapi-290229666Încă nu există evaluări
- Sample Letter To Doc From SchoolDocument3 paginiSample Letter To Doc From Schoolapi-290229666Încă nu există evaluări
- Case Conceptualization AssignmentDocument12 paginiCase Conceptualization Assignmentapi-290229666Încă nu există evaluări
- PsychostimulanthandoutDocument2 paginiPsychostimulanthandoutapi-290229666Încă nu există evaluări
- Determining Math DifficultiesDocument14 paginiDetermining Math Difficultiesapi-290229666Încă nu există evaluări
- Protocol AssignmentDocument3 paginiProtocol Assignmentapi-290229666Încă nu există evaluări
- Ethics CorruptionDocument18 paginiEthics CorruptionJaneÎncă nu există evaluări
- Tcs 3Document2 paginiTcs 3learn2hackÎncă nu există evaluări
- Fluency BibliographyDocument5 paginiFluency Bibliographyapi-320507847Încă nu există evaluări
- Empowerment Technologies: Activity SheetDocument6 paginiEmpowerment Technologies: Activity SheetKEVIN LIBERATOÎncă nu există evaluări
- Zinger - Inquiry AssignmentDocument35 paginiZinger - Inquiry Assignmentapi-375058327Încă nu există evaluări
- Teaching Strategies in MTB 1Document6 paginiTeaching Strategies in MTB 1HASLY NECOLE HASLY LAREZAÎncă nu există evaluări
- A. Pleasure ValuesDocument13 paginiA. Pleasure ValuesGino LacandulaÎncă nu există evaluări
- Years: University of The PhilippinesDocument24 paginiYears: University of The PhilippinesAfricaEdnaÎncă nu există evaluări
- Lesson Plan State ICTDocument2 paginiLesson Plan State ICTVon Glydel MicabaloÎncă nu există evaluări
- Poglodek ResumeDocument1 paginăPoglodek Resumeapi-263447295Încă nu există evaluări
- IS2184 Information Systems ManagementDocument2 paginiIS2184 Information Systems ManagementMihirinie AbhayawardhanaÎncă nu există evaluări
- 169 201516 Syl Babed RieDocument170 pagini169 201516 Syl Babed RieRahul Kumar RamÎncă nu există evaluări
- P3 Introduction 2023 FinalDocument49 paginiP3 Introduction 2023 FinallryuenÎncă nu există evaluări
- What Key Competencies Are Needed in The Digital Age?Document60 paginiWhat Key Competencies Are Needed in The Digital Age?marnekibÎncă nu există evaluări
- Descriptive Lab Report GuideDocument3 paginiDescriptive Lab Report GuideOluwafisayomi LawaniÎncă nu există evaluări
- Essay PWCDocument2 paginiEssay PWCandresuminhÎncă nu există evaluări
- Gcse EssaysDocument3 paginiGcse Essaysafabilalf100% (2)
- Persuasive Text RubricDocument2 paginiPersuasive Text Rubricapi-265914333Încă nu există evaluări
- Remark Results BR705-000084Document2 paginiRemark Results BR705-000084Thiago StechinniÎncă nu există evaluări
- Outstanding TeachersDocument2 paginiOutstanding TeachersKristel Joy ManceraÎncă nu există evaluări
- Ronak Shah 1210Document4 paginiRonak Shah 1210Ronak ShahÎncă nu există evaluări
- University of Kerala: Office of The Controller of ExaminationsDocument1 paginăUniversity of Kerala: Office of The Controller of ExaminationsMerlin KÎncă nu există evaluări
- English Scheme of Work: FORM 3 2020Document5 paginiEnglish Scheme of Work: FORM 3 2020Aizat Zulhilmi YusupÎncă nu există evaluări
- Community Based Ecotourism PDFDocument2 paginiCommunity Based Ecotourism PDFIzhamÎncă nu există evaluări
- T.S. Eliot BiographyDocument2 paginiT.S. Eliot BiographyWeber LiuÎncă nu există evaluări
- Janko Veselinović - Hajduk StankoDocument76 paginiJanko Veselinović - Hajduk StankojocamacaÎncă nu există evaluări
- Letter PahibaloDocument4 paginiLetter PahibaloQueendelyn Eslawan BalabaÎncă nu există evaluări