S-ar putea să vă placă și
- IdentifyinggapsDocument6 paginiIdentifyinggapsapi-426094285Încă nu există evaluări
- Capstone Paper IV Without Submission PacketDocument9 paginiCapstone Paper IV Without Submission Packetapi-484630324Încă nu există evaluări
- Group 1 Draft IIDocument9 paginiGroup 1 Draft IIapi-450475136Încă nu există evaluări
- Capstone Paper Section III Group6 1Document12 paginiCapstone Paper Section III Group6 1api-543045416Încă nu există evaluări
- Sethraheeljong Final PaperDocument13 paginiSethraheeljong Final Paperapi-268623363Încă nu există evaluări
- Nishele Lenards, PHD, CMD, RT (R) (T), FaamdDocument8 paginiNishele Lenards, PHD, CMD, RT (R) (T), Faamdapi-450246598Încă nu există evaluări
- Group 3 Draft 2Document11 paginiGroup 3 Draft 2api-376527663Încă nu există evaluări
- Research Literature Gap Activity - Christina OngDocument4 paginiResearch Literature Gap Activity - Christina Ongapi-396204505Încă nu există evaluări
- Paper Draft3 WipDocument9 paginiPaper Draft3 Wipapi-634067897Încă nu există evaluări
- Final Draft-Formatted12-2-14Document19 paginiFinal Draft-Formatted12-2-14api-237552707Încă nu există evaluări
- BJR 71 846 9849380Document8 paginiBJR 71 846 9849380BitaÎncă nu există evaluări
- Rough Draft 1 - Group 3Document9 paginiRough Draft 1 - Group 3api-376527663Încă nu există evaluări
- Clinical Oncology PaperDocument20 paginiClinical Oncology Paperapi-633111194Încă nu există evaluări
- Draft 1Document7 paginiDraft 1api-267335639Încă nu există evaluări
- RO-ILS Case StudyDocument4 paginiRO-ILS Case Studyapi-458422967Încă nu există evaluări
- Clinical Oncology AssignmentDocument9 paginiClinical Oncology Assignmentapi-691277740Încă nu există evaluări
- Final CompleteDocument11 paginiFinal Completeapi-575843507Încă nu există evaluări
- A Case Study of DIBH To Spare Abdominal Organs at Risk For Renal Cell Carcinoma MR-Guided RadiotherapyDocument14 paginiA Case Study of DIBH To Spare Abdominal Organs at Risk For Renal Cell Carcinoma MR-Guided Radiotherapyapi-525837437Încă nu există evaluări
- Final CapstoneDocument11 paginiFinal Capstoneapi-603721790Încă nu există evaluări
- Research ProposalDocument5 paginiResearch Proposalapi-484630324Încă nu există evaluări
- Treatment Planning ProjectDocument11 paginiTreatment Planning Projectapi-484763634Încă nu există evaluări
- Preoperative Computed Tomography Angiography in Autologous Breast Reconstruction-Incidence and Impact of IncidentalomasDocument6 paginiPreoperative Computed Tomography Angiography in Autologous Breast Reconstruction-Incidence and Impact of IncidentalomasNora Vianey Alcantara VelascoÎncă nu există evaluări
- Evaluation of DIBH Breast Plan Robustness Against Isocenter Positioning UncertaintiesDocument13 paginiEvaluation of DIBH Breast Plan Robustness Against Isocenter Positioning Uncertaintiesapi-484630324Încă nu există evaluări
- Clinical Oncology PaperDocument16 paginiClinical Oncology Paperapi-632529930Încă nu există evaluări
- The Role of The Radiotherapy Technician During Prostate Radiation TreatmentDocument10 paginiThe Role of The Radiotherapy Technician During Prostate Radiation TreatmentFlorian QordjaÎncă nu există evaluări
- Research ProjectDocument16 paginiResearch Projectapi-373572658Încă nu există evaluări
- Research Draft 3 FinalDocument14 paginiResearch Draft 3 Finalapi-299270003Încă nu există evaluări
- Heterogeneity Correction Paper PDF WeeblyDocument16 paginiHeterogeneity Correction Paper PDF Weeblyapi-630263039Încă nu există evaluări
- Abdominoperineal Extralevator ResectionDocument4 paginiAbdominoperineal Extralevator ResectionAnitei GabrielaÎncă nu există evaluări
- Draft4 Researchproject Group8Document18 paginiDraft4 Researchproject Group8api-633248237Încă nu există evaluări
- Research Proposal (Quantitative) Title: Minimizing Clearance Issues With Prone Breast Patients On Varian Linear AcceleratorsDocument4 paginiResearch Proposal (Quantitative) Title: Minimizing Clearance Issues With Prone Breast Patients On Varian Linear Acceleratorsapi-484763634Încă nu există evaluări
- A Dosimetric Comparison of Coplanar vs. Non-Coplanar VMAT SBRT Techniques For NSCLCDocument9 paginiA Dosimetric Comparison of Coplanar vs. Non-Coplanar VMAT SBRT Techniques For NSCLCapi-269672910Încă nu există evaluări
- GapsDocument6 paginiGapsapi-432489466Încă nu există evaluări
- Final DraftDocument15 paginiFinal Draftapi-334402872Încă nu există evaluări
- Final DraftDocument18 paginiFinal Draftapi-334402872Încă nu există evaluări
- Minimizing Clearance Issues With Prone Breast Patients On Varian Linear Accelerators Through Isocenter PlacementDocument18 paginiMinimizing Clearance Issues With Prone Breast Patients On Varian Linear Accelerators Through Isocenter Placementapi-484763634Încă nu există evaluări
- Cancer Paper FinalDocument10 paginiCancer Paper Finalapi-278043011Încă nu există evaluări
- Draft 1Document15 paginiDraft 1api-334402872Încă nu există evaluări
- Final Draft2 Group10 10-24Document24 paginiFinal Draft2 Group10 10-24api-602263051Încă nu există evaluări
- Group 1-Vijay Brittany Pat Seth Veronica Stephanie Sadie Ashley Draft 1Document15 paginiGroup 1-Vijay Brittany Pat Seth Veronica Stephanie Sadie Ashley Draft 1api-334644774Încă nu există evaluări
- Rad Onc II PaperDocument6 paginiRad Onc II Paperapi-277136509Încă nu există evaluări
- Meddos Published ArticleDocument6 paginiMeddos Published Articleapi-350437453Încă nu există evaluări
- Paper Third DraftDocument19 paginiPaper Third Draftapi-405398222Încă nu există evaluări
- What Is The Best Treatment of Malignant Bone Tumors in Children - Clinical GateDocument4 paginiWhat Is The Best Treatment of Malignant Bone Tumors in Children - Clinical GateAkira MasumiÎncă nu există evaluări
- A Comparison of Single-Phase and Phase-Gated Average Verification Plans For Proton RadiotherapyDocument21 paginiA Comparison of Single-Phase and Phase-Gated Average Verification Plans For Proton Radiotherapyapi-645453685Încă nu există evaluări
- TxplanningprojectDocument9 paginiTxplanningprojectapi-432489466Încă nu există evaluări
- Different Styles of IGRTDocument10 paginiDifferent Styles of IGRTPeter CaldwellÎncă nu există evaluări
- Research Paper Conclusion v3 9-25Document22 paginiResearch Paper Conclusion v3 9-25api-602263051Încă nu există evaluări
- Sarcomapaper FinalprogramDocument17 paginiSarcomapaper Finalprogramapi-543045416Încă nu există evaluări
- Resection Probability Maps For Quality Assessment of Glioma Surgery Without Brain Location BiasDocument10 paginiResection Probability Maps For Quality Assessment of Glioma Surgery Without Brain Location BiaspcvdwhÎncă nu există evaluări
- Research Paper Results-Capston IIIDocument21 paginiResearch Paper Results-Capston IIIapi-602263051Încă nu există evaluări
- Effectiveness of A Patient-Specific ImmobilizationDocument12 paginiEffectiveness of A Patient-Specific ImmobilizationHollis LukÎncă nu există evaluări
- Final Complete Group10Document10 paginiFinal Complete Group10api-573564115Încă nu există evaluări
- Final Complete Group10Document10 paginiFinal Complete Group10api-573564115Încă nu există evaluări
- Final Draft6 Group1Document13 paginiFinal Draft6 Group1api-598481829Încă nu există evaluări
- Final Draft6 Group1Document13 paginiFinal Draft6 Group1api-598481829Încă nu există evaluări
- Final Complete Group10Document23 paginiFinal Complete Group10api-573564115Încă nu există evaluări
- Effects of Target Volume Coverage in Superficial Medial and Lateral Breast Tissue Using Flattening Filter-Free BeamsDocument10 paginiEffects of Target Volume Coverage in Superficial Medial and Lateral Breast Tissue Using Flattening Filter-Free Beamsapi-602488644Încă nu există evaluări
- Dose Differences Due To Variance in Contours of The Optic ChiasmDocument15 paginiDose Differences Due To Variance in Contours of The Optic Chiasmapi-527662950Încă nu există evaluări
- Technical Aspects of Focal Therapy in Localized Prostate CancerDe la EverandTechnical Aspects of Focal Therapy in Localized Prostate CancerEric BarretÎncă nu există evaluări
- Oct Nov EvalDocument3 paginiOct Nov Evalapi-268707929Încă nu există evaluări
- Oct Nov EvalDocument3 paginiOct Nov Evalapi-268707929Încă nu există evaluări
- H N ImrtDocument2 paginiH N Imrtapi-268707929Încă nu există evaluări
- Oct Nov EvalDocument3 paginiOct Nov Evalapi-268707929Încă nu există evaluări
- Psi CompDocument3 paginiPsi Compapi-268707929Încă nu există evaluări
- Oct Nov EvalDocument3 paginiOct Nov Evalapi-268707929Încă nu există evaluări
- Fall Case Log TotalsDocument2 paginiFall Case Log TotalsBen LemieuxÎncă nu există evaluări
- Sample BudgetDocument6 paginiSample Budgetapi-268707929Încă nu există evaluări
- Case Log IIDocument2 paginiCase Log IIapi-268707929Încă nu există evaluări
- Oct Nov EvalDocument3 paginiOct Nov Evalapi-268707929Încă nu există evaluări
- Sept EvalDocument3 paginiSept Evalapi-268707929Încă nu există evaluări
- Case Study Clinical Prac 3Document8 paginiCase Study Clinical Prac 3api-268707929Încă nu există evaluări
- Oct Nov EvalDocument3 paginiOct Nov Evalapi-268707929Încă nu există evaluări
- Oct Nov EvalDocument3 paginiOct Nov Evalapi-268707929Încă nu există evaluări
- Budget ActivityDocument2 paginiBudget Activityapi-247490129Încă nu există evaluări
- Yasmin Final PaperDocument10 paginiYasmin Final Paperapi-268707929Încă nu există evaluări
- Job DescDocument2 paginiJob Descapi-268707929Încă nu există evaluări
- Comp 2 NdsemesterDocument3 paginiComp 2 Ndsemesterapi-268707929Încă nu există evaluări
- Edited Citation AssignmentDocument1 paginăEdited Citation Assignmentapi-268707929Încă nu există evaluări
- JunejulyevalDocument3 paginiJunejulyevalapi-268707929Încă nu există evaluări
- CompiiDocument3 paginiCompiiapi-268707929Încă nu există evaluări
- MentoringyasminfinalDocument7 paginiMentoringyasminfinalapi-268707929Încă nu există evaluări
- JulyaugustevalDocument3 paginiJulyaugustevalapi-268707929Încă nu există evaluări
- Csi ProjectDocument7 paginiCsi Projectapi-268707929Încă nu există evaluări
- Photon CompDocument3 paginiPhoton Compapi-268707929Încă nu există evaluări
- Service Learning Project IIDocument7 paginiService Learning Project IIapi-268707929Încă nu există evaluări
- Parotid LabDocument11 paginiParotid Labapi-268707929Încă nu există evaluări
- MayjuneDocument3 paginiMayjuneapi-268707929Încă nu există evaluări
- Case LogDocument2 paginiCase Logapi-268707929Încă nu există evaluări
- Astm d4945Document7 paginiAstm d4945M.Malyadri ReddyÎncă nu există evaluări
- Ferro CementDocument236 paginiFerro Cementpbharadwaj545Încă nu există evaluări
- Paper - Fatigue Lifetime of Welded Joints Under Random Loading - Colombini P., Dolinski K. - 2001Document11 paginiPaper - Fatigue Lifetime of Welded Joints Under Random Loading - Colombini P., Dolinski K. - 2001Claudio RodriguesÎncă nu există evaluări
- Experimental Physics PDFDocument2 paginiExperimental Physics PDFJessicaÎncă nu există evaluări
- DIP Lecture 1&2 PDFDocument63 paginiDIP Lecture 1&2 PDFAhmedÎncă nu există evaluări
- DEWA Regulations For Electrical Installations 2017 Edition PDFDocument135 paginiDEWA Regulations For Electrical Installations 2017 Edition PDFakhilÎncă nu există evaluări
- Delta Industrial Articulated Robot SeriesDocument15 paginiDelta Industrial Articulated Robot Seriesrobotech automationÎncă nu există evaluări
- Reactor Design For Cell GrothDocument33 paginiReactor Design For Cell GrothErpin FebrianÎncă nu există evaluări
- Lifetime Calculation of Irregularly Oscillating Bearings in Offshore WinchesDocument12 paginiLifetime Calculation of Irregularly Oscillating Bearings in Offshore WinchesNadav SharabiÎncă nu există evaluări
- Firewater Hydraulic Study Report Detailed Engineering Design Oml-24 Crude Storage Tanks and De-Watering ProjectDocument22 paginiFirewater Hydraulic Study Report Detailed Engineering Design Oml-24 Crude Storage Tanks and De-Watering ProjectPatrick AyanÎncă nu există evaluări
- Several Problems of The Polish Physics Olympiad: Waldemar GorzkowskiDocument4 paginiSeveral Problems of The Polish Physics Olympiad: Waldemar GorzkowskiVikram SaurabhÎncă nu există evaluări
- Phy1 11 - 12 Q1 0102 FDDocument31 paginiPhy1 11 - 12 Q1 0102 FDKaye AquinoÎncă nu există evaluări
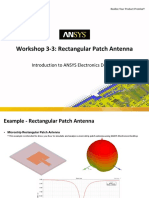
- Workshop 3-3: Rectangular Patch Antenna: Introduction To ANSYS Electronics DesktopDocument21 paginiWorkshop 3-3: Rectangular Patch Antenna: Introduction To ANSYS Electronics DesktopRodrigoÎncă nu există evaluări
- MEF University Math 115 Calculus Fall 2018-19 Midterm Exam 1 2 3 4 PDocument4 paginiMEF University Math 115 Calculus Fall 2018-19 Midterm Exam 1 2 3 4 PMELİHA KOÇÎncă nu există evaluări
- ASCE710E1Document40 paginiASCE710E1Tabish Islam100% (2)
- Tolerances and FitsDocument12 paginiTolerances and FitskoitkulperÎncă nu există evaluări
- 50 Questions and Answers For Marine Engineers: Issue 3Document10 pagini50 Questions and Answers For Marine Engineers: Issue 3Tara Gonzales100% (3)
- Pre-Admission Math Assessment - SampleDocument13 paginiPre-Admission Math Assessment - SamplePranav BISUMBHERÎncă nu există evaluări
- 2010 Aisc Steel ToolsDocument4 pagini2010 Aisc Steel Toolsmuh2006Încă nu există evaluări
- Development of A Belt Conveyor For Small Scale Industry: September 2017Document6 paginiDevelopment of A Belt Conveyor For Small Scale Industry: September 2017DatÎncă nu există evaluări
- CPRF Analysis PDFDocument8 paginiCPRF Analysis PDFMohd FirojÎncă nu există evaluări
- Acid Base SeparationDocument6 paginiAcid Base SeparationAlexandra CatalinaÎncă nu există evaluări
- ENGINEERING - MATHEMATICS - 2 VTU Syllabus PDFDocument167 paginiENGINEERING - MATHEMATICS - 2 VTU Syllabus PDFAdarshÎncă nu există evaluări
- 0i Connection Manual 64113EN1 PDFDocument1.224 pagini0i Connection Manual 64113EN1 PDFAnkit SabhayaÎncă nu există evaluări
- Unit Plan M7 S.Y. 2020 2021Document14 paginiUnit Plan M7 S.Y. 2020 2021dan teÎncă nu există evaluări
- Crop CircleDocument2 paginiCrop CircledotionmoÎncă nu există evaluări
- Kids Math - Angles Glossary and TermsDocument7 paginiKids Math - Angles Glossary and Termssathish11407144Încă nu există evaluări
- As 60034.22-2010 Rotating Electrical Machines AC Generators For Reciprocating Internal Combustion (RIC) EnginDocument8 paginiAs 60034.22-2010 Rotating Electrical Machines AC Generators For Reciprocating Internal Combustion (RIC) EnginSAI Global - APAC100% (1)
- Biography: Aryabhata (IAST: Āryabhaṭa; Sanskrit: आयरभटः) (476-550 CE) was the first in theDocument7 paginiBiography: Aryabhata (IAST: Āryabhaṭa; Sanskrit: आयरभटः) (476-550 CE) was the first in theshabaan786Încă nu există evaluări
- Flint-2 5Document671 paginiFlint-2 5GNZLÎncă nu există evaluări