S-ar putea să vă placă și
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDe la EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesEvaluare: 4 din 5 stele4/5 (2)
- 11 15Document8 pagini11 15Dinarkram Rabreca EculÎncă nu există evaluări
- Drug Study For Mefenamic Acid, Tramadol and CefuroximeDocument7 paginiDrug Study For Mefenamic Acid, Tramadol and CefuroximeChristian Karl B. LlanesÎncă nu există evaluări
- DRUG STUDY AND SOAPIE SUBMITTEDDocument17 paginiDRUG STUDY AND SOAPIE SUBMITTEDYasi EcheniqueÎncă nu există evaluări
- All Kinds of DrugsDocument11 paginiAll Kinds of DrugsRene John Francisco100% (1)
- AmoxicillinDocument2 paginiAmoxicillindheng05Încă nu există evaluări
- Pharma Cards.Document19 paginiPharma Cards.Brent NicholsÎncă nu există evaluări
- C C C Vertigo,: Electrolyte and Water Balance AgentDocument12 paginiC C C Vertigo,: Electrolyte and Water Balance AgentEarl Tony TrinidadÎncă nu există evaluări
- Relief of gas and bloatingDocument6 paginiRelief of gas and bloatingMichael John Gambong SalaÎncă nu există evaluări
- Ncp&drugstudDocument12 paginiNcp&drugstudSarah Mae Billano BermudezÎncă nu există evaluări
- Ranitidine, Acetaminophen, Albuterol Drug StudyDocument5 paginiRanitidine, Acetaminophen, Albuterol Drug StudyBea Andrea LarismaÎncă nu există evaluări
- Drug Study ShenDocument12 paginiDrug Study ShenLass KazeÎncă nu există evaluări
- Fluvoxamine MaleateDocument3 paginiFluvoxamine MaleateHilman Fitriaji Suganda PrawiraÎncă nu există evaluări
- Ventolin Nebulizer for Bronchospasm ReliefDocument10 paginiVentolin Nebulizer for Bronchospasm ReliefmidskiescreamzÎncă nu există evaluări
- Gabapentin medication guideDocument15 paginiGabapentin medication guideTyron ChuaÎncă nu există evaluări
- Paracetamol Antipyretic and Analgesic GuideDocument7 paginiParacetamol Antipyretic and Analgesic GuideAnne Monique Moran OngjocoÎncă nu există evaluări
- Neuropathic Pain Diabetic Peripheral NeuropathyDocument7 paginiNeuropathic Pain Diabetic Peripheral NeuropathyJomabee TuArÎncă nu există evaluări
- Therapeutic: Urinary Tract Stimulants Pharmacologic: CholinergicDocument37 paginiTherapeutic: Urinary Tract Stimulants Pharmacologic: CholinergicApple MaeÎncă nu există evaluări
- Drug Study HydralazineDocument10 paginiDrug Study HydralazineLuige AvilaÎncă nu există evaluări
- Side Effects:: AtropineDocument7 paginiSide Effects:: AtropinekletadaÎncă nu există evaluări
- Cefuroxime Drug AnaDocument4 paginiCefuroxime Drug AnaCarpz DarpzÎncă nu există evaluări
- Psych Drug StudyDocument5 paginiPsych Drug StudyLorina Lynne Apelacio100% (4)
- Adults and Children 15 Y Pediatric 6 - 14 YDocument2 paginiAdults and Children 15 Y Pediatric 6 - 14 YFildehl Janice Bomediano Catipay100% (1)
- Drug Study 2Document8 paginiDrug Study 2rey_tengÎncă nu există evaluări
- Sim 4Document4 paginiSim 4Ding EmilyÎncă nu există evaluări
- ANTIPSYCHOTICS Olanzapine (Zyprexa), Aripiprazole (Abilify), Chlorpromazine (Thorazine)Document5 paginiANTIPSYCHOTICS Olanzapine (Zyprexa), Aripiprazole (Abilify), Chlorpromazine (Thorazine)Rhanne BolanteÎncă nu există evaluări
- ImipramineDocument6 paginiImipramineMuhammed Faruk JambazÎncă nu există evaluări
- AnalgesicDocument3 paginiAnalgesicAnnaMaeVelosoÎncă nu există evaluări
- Drug Name Classification and Mechanism of Action Indication/ Dosage/ Route Contraindicatio N Adverse Effects Nursing InterventionsDocument6 paginiDrug Name Classification and Mechanism of Action Indication/ Dosage/ Route Contraindicatio N Adverse Effects Nursing InterventionsVin LandichoÎncă nu există evaluări
- Emergency Drugs Drug StudyDocument15 paginiEmergency Drugs Drug StudyCathrine Sandile Tangwara100% (1)
- Drug StudyDocument9 paginiDrug StudyChristine PunsalanÎncă nu există evaluări
- COPD Drug Study: Ipratropium Bromide and Albuterol SulfateDocument9 paginiCOPD Drug Study: Ipratropium Bromide and Albuterol SulfateShane Arroyo100% (1)
- Chlorpromazine Dosage GuideDocument3 paginiChlorpromazine Dosage GuideChristine Pialan SalimbagatÎncă nu există evaluări
- COPD Medications Reduce Inflammation Improve BreathingDocument3 paginiCOPD Medications Reduce Inflammation Improve BreathingKdamnzÎncă nu există evaluări
- Psychia Drug StudyDocument11 paginiPsychia Drug StudyJustin 葉志明 Yap Delapaz100% (1)
- Drug Study FORTDocument3 paginiDrug Study FORTLysa Mae EleazarÎncă nu există evaluări
- Clonazepam KlonopinDocument3 paginiClonazepam KlonopinKristi WrayÎncă nu există evaluări
- Drug-Study-Po (1) EwesdfdsfdsfsddsfdsfdsDocument14 paginiDrug-Study-Po (1) EwesdfdsfdsfsddsfdsfdsIbrahim RegachoÎncă nu există evaluări
- Drug Study ON Cabergolin EDocument4 paginiDrug Study ON Cabergolin ESimran SimzÎncă nu există evaluări
- Emergency DrugsDocument15 paginiEmergency Drugsjheverly123100% (1)
- Drug Study On Emergency DrugsDocument16 paginiDrug Study On Emergency DrugsJosepÎncă nu există evaluări
- Drug Study On Emergency DrugsDocument15 paginiDrug Study On Emergency DrugsJAy TootÎncă nu există evaluări
- Drug Studies PsychDocument12 paginiDrug Studies PsychAnna Mendiola-BasbasÎncă nu există evaluări
- Epinephrine: Uses, Dosages, Side EffectsDocument15 paginiEpinephrine: Uses, Dosages, Side EffectsDennise Juayang100% (1)
- Drug Study-Grand Case PresDocument8 paginiDrug Study-Grand Case PresLorina Lynne ApelacioÎncă nu există evaluări
- ZafirlukastDocument3 paginiZafirlukastapi-379794167% (3)
- Drugs Study Pedia PDFDocument8 paginiDrugs Study Pedia PDFmark angeloÎncă nu există evaluări
- Zyprexa: Generic Name: OlanzapineDocument3 paginiZyprexa: Generic Name: Olanzapinenasir khanÎncă nu există evaluări
- ZileutonDocument3 paginiZileutonapi-3797941100% (2)
- Calcium Carbonate for Bone HealthDocument14 paginiCalcium Carbonate for Bone HealthBianca Freya Porral85% (13)
- Managing pain with TramadolDocument3 paginiManaging pain with TramadolMicaela Andrea CieloÎncă nu există evaluări
- Drugs Study For PneumoniaDocument5 paginiDrugs Study For PneumoniaLucelle ArellanoÎncă nu există evaluări
- Drug StudyDocument9 paginiDrug StudyShiara Ruth EdrosoloÎncă nu există evaluări
- Olanzapine C Loza Pine, Drug StudyDocument7 paginiOlanzapine C Loza Pine, Drug StudyAubrey MacÎncă nu există evaluări
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcDe la EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcÎncă nu există evaluări
- Fast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonDe la EverandFast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonÎncă nu există evaluări
- ChartingDocument1 paginăChartingkotonashiÎncă nu există evaluări
- KardexDocument2 paginiKardexkotonashiÎncă nu există evaluări
- NCP FormatDocument2 paginiNCP FormatkotonashiÎncă nu există evaluări
- NCP FormatDocument2 paginiNCP FormatkotonashiÎncă nu există evaluări
- Patofisiologi FibroadenomaDocument2 paginiPatofisiologi FibroadenomaMalinda Priskasari0% (1)
- Schizophrenia ResidualDocument12 paginiSchizophrenia ResidualkotonashiÎncă nu există evaluări
- FHPformatDocument2 paginiFHPformatkotonashiÎncă nu există evaluări
- MCQ I II Psych 2 PDFDocument19 paginiMCQ I II Psych 2 PDFSpacetoon DaysÎncă nu există evaluări
- MELODY 5.3 Treatment Methods Theoretical - V2.0 - 211122Document19 paginiMELODY 5.3 Treatment Methods Theoretical - V2.0 - 211122MelodyÎncă nu există evaluări
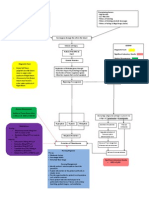
- Esophagus Diseases and SymptomsDocument60 paginiEsophagus Diseases and SymptomsSalma NajjarÎncă nu există evaluări
- NCM 114 Care For Older Adults MODULE 4Document5 paginiNCM 114 Care For Older Adults MODULE 4Meryville JacildoÎncă nu există evaluări
- Public Health Situation Analysis SOPsDocument42 paginiPublic Health Situation Analysis SOPsI Gusti Ayu Adinda Dewi Prativi DindaÎncă nu există evaluări
- IX. Discharge PlanDocument2 paginiIX. Discharge PlanAlfrien Ivanovich LarchsonÎncă nu există evaluări
- National Tuberculosis Program: Valenzuela City Accomplishment 2018-2019-2020Document43 paginiNational Tuberculosis Program: Valenzuela City Accomplishment 2018-2019-2020JohnPhilipTiongcoÎncă nu există evaluări
- Understanding India's Infrastructure ChallengesDocument23 paginiUnderstanding India's Infrastructure ChallengesDhruv GuptaÎncă nu există evaluări
- BTS Guideline For Oxygen Use in Adults in HealthcareDocument89 paginiBTS Guideline For Oxygen Use in Adults in HealthcareSoto BrissetteÎncă nu există evaluări
- Respiratory System Anatomy and DiseasesDocument25 paginiRespiratory System Anatomy and DiseasesDaniellaÎncă nu există evaluări
- Plastic and the Environment - SEO Optimized TitleDocument110 paginiPlastic and the Environment - SEO Optimized TitleThị HồngÎncă nu există evaluări
- Golden RetrieverDocument77 paginiGolden RetrieverAlfred AdeniyiÎncă nu există evaluări
- Recurrent Fever Case StudyDocument3 paginiRecurrent Fever Case StudymroxandeeÎncă nu există evaluări
- Stroke 2020 Continuum PDFDocument195 paginiStroke 2020 Continuum PDFMazin Al-Tahir100% (1)
- Synopsis-Of-Psychiatry BarlowDocument13 paginiSynopsis-Of-Psychiatry BarlowKylle Kayser CanlasÎncă nu există evaluări
- Parameters of Quality ControlDocument36 paginiParameters of Quality ControlAngelo Jude CobachaÎncă nu există evaluări
- 10 Tips To Prevent Spreading Impetigo, and Avoid Getting It AgainDocument2 pagini10 Tips To Prevent Spreading Impetigo, and Avoid Getting It Againputri aisheÎncă nu există evaluări
- DPL OperationDocument2 paginiDPL OperationTao JunÎncă nu există evaluări
- Scaitic Treatment PDFDocument5 paginiScaitic Treatment PDFSebastiano SerraÎncă nu există evaluări
- CDC Clear Communication Index: User GuideDocument36 paginiCDC Clear Communication Index: User GuideJesse ManekÎncă nu există evaluări
- Diabetes-Knowledge-Test Page-1-To-10Document31 paginiDiabetes-Knowledge-Test Page-1-To-10api-559575515Încă nu există evaluări
- Post Traumatic Stress Disorder PTSD FactsheetDocument26 paginiPost Traumatic Stress Disorder PTSD Factsheethalima mahmoodÎncă nu există evaluări
- Star Health Assure - One Pager - Version 1.0 - April - 2022Document3 paginiStar Health Assure - One Pager - Version 1.0 - April - 2022Shihb100% (1)
- Myhealth Suraksha-Policy WordingDocument39 paginiMyhealth Suraksha-Policy Wordingjio325113Încă nu există evaluări
- Community DiagnosisDocument164 paginiCommunity DiagnosisYabetsÎncă nu există evaluări
- 1365-Article Text-8141-1-4-20210610Document16 pagini1365-Article Text-8141-1-4-20210610Maabena AsanteÎncă nu există evaluări
- Catalog Snibe Maglumi 800 English PDFDocument7 paginiCatalog Snibe Maglumi 800 English PDFAniket DubeyÎncă nu există evaluări
- Huntington's DiseaseDocument9 paginiHuntington's DiseaseBARATHY A/P RAMAN KPM-GuruÎncă nu există evaluări
- Impact of Malnutrition On Immunity and InfectionDocument17 paginiImpact of Malnutrition On Immunity and InfectionYusuf NugrohoÎncă nu există evaluări
- Lip BumperDocument60 paginiLip BumperPînzariu GeorgeÎncă nu există evaluări