S-ar putea să vă placă și
- Pat Fall 2014Document17 paginiPat Fall 2014api-300849832Încă nu există evaluări
- Pat 2014Document20 paginiPat 2014api-324658071Încă nu există evaluări
- Pat 2 Medsurg 2Document22 paginiPat 2 Medsurg 2api-315731045Încă nu există evaluări
- Pat 2 sd-1Document22 paginiPat 2 sd-1api-283672381Încă nu există evaluări
- Pat Med Surg 1Document22 paginiPat Med Surg 1api-324658071Încă nu există evaluări
- Pat Revised 9-2014 FundamentalsDocument17 paginiPat Revised 9-2014 Fundamentalsapi-300362033Încă nu există evaluări
- Pat MsiiDocument21 paginiPat Msiiapi-324658071Încă nu există evaluări
- Pat Revised 2013 1Document23 paginiPat Revised 2013 1api-314062228Încă nu există evaluări
- Alegrias Pat-FundsDocument14 paginiAlegrias Pat-Fundsapi-324006383Încă nu există evaluări
- Ms 2 Pat MaffettDocument20 paginiMs 2 Pat Maffettapi-339784339Încă nu există evaluări
- Ms 1 PatDocument19 paginiMs 1 Patapi-281676750Încă nu există evaluări
- Msii Pat 2Document22 paginiMsii Pat 2api-300946501Încă nu există evaluări
- Pat Semester 1Document17 paginiPat Semester 1api-300946501Încă nu există evaluări
- Pat 1 2015Document18 paginiPat 1 2015api-315192697Încă nu există evaluări
- Pat II MedsurgDocument19 paginiPat II Medsurgapi-301881424Încă nu există evaluări
- Pat Spring Ms II 2015Document16 paginiPat Spring Ms II 2015api-315435865Încă nu există evaluări
- Jones PatDocument16 paginiJones Patapi-301978768Încă nu există evaluări
- Patsummersemester2015 Anjouligerez-2Document21 paginiPatsummersemester2015 Anjouligerez-2api-325112936Încă nu există evaluări
- Pat FundamentalsDocument16 paginiPat Fundamentalsapi-339980385Încă nu există evaluări
- Pat 2 - Med SurgDocument21 paginiPat 2 - Med Surgapi-315731045Încă nu există evaluări
- Pat Ms IIDocument18 paginiPat Ms IIapi-339980385Încă nu există evaluări
- Med Surg 2 Pat 1Document24 paginiMed Surg 2 Pat 1api-315444338Încă nu există evaluări
- Pat Fall 2014Document21 paginiPat Fall 2014api-288536467Încă nu există evaluări
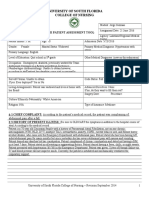
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument18 paginiUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-340518534Încă nu există evaluări
- Patient Assessment Tool ms2Document27 paginiPatient Assessment Tool ms2api-280998981Încă nu există evaluări
- Fundamentals PatDocument20 paginiFundamentals Patapi-340247560Încă nu există evaluări
- Pat FinalDocument24 paginiPat Finalapi-252804976Încă nu există evaluări
- Pat1 Med Surg 1Document19 paginiPat1 Med Surg 1api-339132978Încă nu există evaluări
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument17 paginiUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-340518534Încă nu există evaluări
- Pat 3Document21 paginiPat 3api-272761526Încă nu există evaluări
- University of South Florida College of Nursing: Fundamental Patient Assessment ToolDocument18 paginiUniversity of South Florida College of Nursing: Fundamental Patient Assessment Toolapi-315731045Încă nu există evaluări
- Pat 1 Medsurg 2Document18 paginiPat 1 Medsurg 2api-294300618Încă nu există evaluări
- Pat Med Surg IDocument22 paginiPat Med Surg Iapi-302664008Încă nu există evaluări
- Portfolio Pat 3Document19 paginiPortfolio Pat 3api-300861055Încă nu există evaluări
- Pat Revised 2013 1Document18 paginiPat Revised 2013 1api-324886317Încă nu există evaluări
- Pat 2 Medsurg1Document20 paginiPat 2 Medsurg1api-300849832Încă nu există evaluări
- Maffett Fundamentals Pat 2015Document16 paginiMaffett Fundamentals Pat 2015api-339784339Încă nu există evaluări
- ms1 PatDocument17 paginims1 Patapi-325271731Încă nu există evaluări
- Pat DHDocument17 paginiPat DHapi-283153247Încă nu există evaluări
- Pat 2 Med Surg - Dean GradedDocument24 paginiPat 2 Med Surg - Dean Gradedapi-252790184Încă nu există evaluări
- Pat Msii November 2015Document20 paginiPat Msii November 2015api-301120253Încă nu există evaluări
- Pat 3rd SemesterDocument19 paginiPat 3rd Semesterapi-324006383Încă nu există evaluări
- Pat 2Document20 paginiPat 2api-300362983Încă nu există evaluări
- DocDocument19 paginiDocapi-325122079Încă nu există evaluări
- Pat 2Document18 paginiPat 2api-273138891Încă nu există evaluări
- Pat 2 Med SurgDocument18 paginiPat 2 Med Surgapi-316861395Încă nu există evaluări
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument20 paginiUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-300454618Încă nu există evaluări
- Pat Medsurg1Document22 paginiPat Medsurg1api-302151448Încă nu există evaluări
- Pat 11052014Document18 paginiPat 11052014api-300362983Încă nu există evaluări
- Pat Revised 2013 1Document19 paginiPat Revised 2013 1api-300362033Încă nu există evaluări
- ms2 Pat2Document22 paginims2 Pat2api-315588288Încă nu există evaluări
- Pat PortfolioDocument24 paginiPat Portfolioapi-283407010Încă nu există evaluări
- Pat PortfolioDocument20 paginiPat Portfolioapi-300861055Încă nu există evaluări
- Childhood AsthmaDocument53 paginiChildhood AsthmaOlulode Olufemi S100% (1)
- Community Medicine Department Faculty of Medicine University of Indonesia Setyawati Budiningsih, Retno Asti Werdhani Nuri Purwito Adi April 4th 2012Document60 paginiCommunity Medicine Department Faculty of Medicine University of Indonesia Setyawati Budiningsih, Retno Asti Werdhani Nuri Purwito Adi April 4th 2012Faridah Yuwono 28Încă nu există evaluări
- Evidence-Based Case Report: Group A3Document12 paginiEvidence-Based Case Report: Group A3prininditaÎncă nu există evaluări
- Pat2 Med Surg 2Document19 paginiPat2 Med Surg 2api-339132978Încă nu există evaluări
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument22 paginiUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-300454618Încă nu există evaluări
- Screening For Good Health: The Australian Guide To Health Screening And ImmunisationDe la EverandScreening For Good Health: The Australian Guide To Health Screening And ImmunisationÎncă nu există evaluări
- Projectnurse UsfDocument7 paginiProjectnurse Usfapi-300861055Încă nu există evaluări
- Projectnurse Usf Final EvalDocument7 paginiProjectnurse Usf Final Evalapi-300861055Încă nu există evaluări
- Projectnurse Usf FundamentalsDocument19 paginiProjectnurse Usf Fundamentalsapi-300861055Încă nu există evaluări
- K SheltonDocument1 paginăK Sheltonapi-300861055Încă nu există evaluări
- Clinical ExemplarDocument5 paginiClinical Exemplarapi-300861055Încă nu există evaluări
- PSQCM Project No AudioDocument11 paginiPSQCM Project No Audioapi-300861055Încă nu există evaluări
- Ahec CertificationDocument1 paginăAhec Certificationapi-300861055Încă nu există evaluări
- Capstone Summative PortfolioDocument13 paginiCapstone Summative Portfolioapi-300861055Încă nu există evaluări
- Va Cover LetterDocument1 paginăVa Cover Letterapi-300861055Încă nu există evaluări
- Non Va ResumeDocument1 paginăNon Va Resumeapi-300861055Încă nu există evaluări
- Portfolio Pat 3Document19 paginiPortfolio Pat 3api-300861055Încă nu există evaluări
- Ebp Synthesis PortfolioDocument9 paginiEbp Synthesis Portfolioapi-300861055Încă nu există evaluări
- Pat PortfolioDocument20 paginiPat Portfolioapi-300861055Încă nu există evaluări
- DC-DC Converter Reliability Design and TestingDocument16 paginiDC-DC Converter Reliability Design and TestinggirisanaÎncă nu există evaluări
- Karakteristik Morfologik Kambing Spesifik Lokal Di Kabupaten Samosir Sumatera UtaraDocument6 paginiKarakteristik Morfologik Kambing Spesifik Lokal Di Kabupaten Samosir Sumatera UtaraOlivia SimanungkalitÎncă nu există evaluări
- A History Analysis and Performance Guide To Samuel Barber?Document117 paginiA History Analysis and Performance Guide To Samuel Barber?giorgio planesioÎncă nu există evaluări
- Dr. Sun Chemistry Summary 2019 PDFDocument75 paginiDr. Sun Chemistry Summary 2019 PDFPranav ChatiÎncă nu există evaluări
- How To Love The LORD With All Your Heart, Soul, and StrengthDocument5 paginiHow To Love The LORD With All Your Heart, Soul, and StrengthGodmadeMusic100% (1)
- DualSPHysics v4.0 GUIDE PDFDocument140 paginiDualSPHysics v4.0 GUIDE PDFFelipe A Maldonado GÎncă nu există evaluări
- Chapter 8Document3 paginiChapter 8sasafoadjeiÎncă nu există evaluări
- Current Communist CountriesDocument4 paginiCurrent Communist CountriesJJ MGÎncă nu există evaluări
- 2012 C R I M I N A L L A W 1 Reviewer Wordpresscom 5a237cee1723dd6eef7c227dDocument15 pagini2012 C R I M I N A L L A W 1 Reviewer Wordpresscom 5a237cee1723dd6eef7c227dSan PedroÎncă nu există evaluări
- 22-Submission File-35-1-10-20190811Document3 pagini22-Submission File-35-1-10-20190811DhevÎncă nu există evaluări
- Copyright Protection for TV Show FormatsDocument11 paginiCopyright Protection for TV Show FormatsJoy Navaja DominguezÎncă nu există evaluări
- Executive Summary WynnDocument5 paginiExecutive Summary Wynnapi-505730347Încă nu există evaluări
- Report Anomalies and Normalization SummaryDocument5 paginiReport Anomalies and Normalization SummaryThomas_GodricÎncă nu există evaluări
- English (Step Ahead)Document33 paginiEnglish (Step Ahead)ry4nek4100% (1)
- Practical 1Document3 paginiPractical 1Paulus DorlenÎncă nu există evaluări
- 211 - Organizational Behaviour-Pearson Education Limited (2020)Document5 pagini211 - Organizational Behaviour-Pearson Education Limited (2020)mozam haqÎncă nu există evaluări
- Chara LesDocument5 paginiChara Lesx456456456xÎncă nu există evaluări
- Xerox 6030 PDFDocument663 paginiXerox 6030 PDFРумен ИвановÎncă nu există evaluări
- Advantage and Disadvantage Bode PlotDocument2 paginiAdvantage and Disadvantage Bode PlotJohan Sulaiman33% (3)
- Crane's Manual - CV ValuesDocument14 paginiCrane's Manual - CV Valuesnghiemta18Încă nu există evaluări
- 2 10 1 PBDocument4 pagini2 10 1 PBHeesung KimÎncă nu există evaluări
- CHN ReviewerDocument9 paginiCHN ReviewerAnonymousTargetÎncă nu există evaluări
- Recovering Mind and Body (Mental Health)Document24 paginiRecovering Mind and Body (Mental Health)Shivamani143100% (1)
- 50 Important Quotes You Should Pay Attention To in Past The Shallows Art of Smart EducationDocument12 pagini50 Important Quotes You Should Pay Attention To in Past The Shallows Art of Smart EducationSailesh VeluriÎncă nu există evaluări
- History of English - IntroductionDocument58 paginiHistory of English - IntroductionPaul Edward GuevarraÎncă nu există evaluări
- Case: Macariola Vs AsuncionDocument18 paginiCase: Macariola Vs Asuncionjica GulaÎncă nu există evaluări
- Balay Dako Menu DigitalDocument27 paginiBalay Dako Menu DigitalCarlo -Încă nu există evaluări
- Reporter Matt Rudd Goes On An Extraordinary Plane RideDocument2 paginiReporter Matt Rudd Goes On An Extraordinary Plane RideHAnhh TrầnnÎncă nu există evaluări
- Grade 5 DLL SCIENCE 5 Q4 Week 9Document6 paginiGrade 5 DLL SCIENCE 5 Q4 Week 9Joanna Marie Cruz FelipeÎncă nu există evaluări
- New Dll-Math Week 4-1Document3 paginiNew Dll-Math Week 4-1AstroÎncă nu există evaluări