S-ar putea să vă placă și
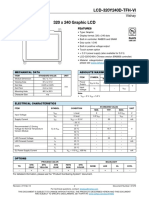
- LCD 320 y 240 DtfhviDocument20 paginiLCD 320 y 240 DtfhviNguyen ThuanÎncă nu există evaluări
- Upload 00030534 1668153449841Document5 paginiUpload 00030534 1668153449841Nguyen ThuanÎncă nu există evaluări
- A61628 ss500 AG enDocument162 paginiA61628 ss500 AG enNguyen ThuanÎncă nu există evaluări
- Agfa NXDocument12 paginiAgfa NXOmar Stalin Lucio Ron50% (2)
- Teaching DR/CR Best Dose PracticesDocument31 paginiTeaching DR/CR Best Dose PracticesNguyen ThuanÎncă nu există evaluări
- Trimax CR MachineDocument55 paginiTrimax CR MachineNguyen ThuanÎncă nu există evaluări
- Grid 1000Document2 paginiGrid 1000Nguyen ThuanÎncă nu există evaluări
- C-DR Training PDFDocument34 paginiC-DR Training PDFNguyen ThuanÎncă nu există evaluări
- I Ns Truc Tio NDocument1 paginăI Ns Truc Tio NNguyen ThuanÎncă nu există evaluări
- 2-9 - 4 Carestream Gridded CassetteDocument2 pagini2-9 - 4 Carestream Gridded CassetteNguyen ThuanÎncă nu există evaluări
- EC CertificationDocument3 paginiEC CertificationNguyen ThuanÎncă nu există evaluări
- B1 Ch?y File KB3020369 B2 Ch?y File KB2533623 B3 Ch?y Xperia CompanionDocument1 paginăB1 Ch?y File KB3020369 B2 Ch?y File KB2533623 B3 Ch?y Xperia CompanionNguyen ThuanÎncă nu există evaluări
- Carestream Vita CR System User GuieDocument116 paginiCarestream Vita CR System User GuieLuis Lara0% (1)
- Extreme User ManualDocument72 paginiExtreme User ManualMohsin LatifÎncă nu există evaluări
- Pretest CDHAYHDocument1 paginăPretest CDHAYHNguyen ThuanÎncă nu există evaluări
- LogDocument2 paginiLogVillalana LabonteÎncă nu există evaluări
- X-Ray Diffraction Simulation Using Laser Pointers and PrintersDocument5 paginiX-Ray Diffraction Simulation Using Laser Pointers and PrintersNguyen ThuanÎncă nu există evaluări
- X-Ray Diffraction Simulation Using Laser Pointers and PrintersDocument5 paginiX-Ray Diffraction Simulation Using Laser Pointers and PrintersNguyen ThuanÎncă nu există evaluări
- Solutions Introduction To Signal ProcessingDocument148 paginiSolutions Introduction To Signal ProcessingCường Phan100% (4)
- English Grammar in Use Extra Cd-Rom ReadmeDocument6 paginiEnglish Grammar in Use Extra Cd-Rom ReadmeLong Nguyễn HoàngÎncă nu există evaluări
- English Grammar in Use Extra Cd-Rom ReadmeDocument6 paginiEnglish Grammar in Use Extra Cd-Rom ReadmeLong Nguyễn HoàngÎncă nu există evaluări
- Solutions Introduction To Signal ProcessingDocument148 paginiSolutions Introduction To Signal ProcessingCường Phan100% (4)
- Calculating Determinants of Square MatricesDocument3 paginiCalculating Determinants of Square MatricesNguyen ThuanÎncă nu există evaluări
- Calculating The DeterminantDocument3 paginiCalculating The DeterminantNguyen ThuanÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Baptism in The Holy SpiritDocument65 paginiBaptism in The Holy SpiritMICHAEL OMONDIÎncă nu există evaluări
- Violent Extremism in South AfricaDocument20 paginiViolent Extremism in South AfricaMulidsahayaÎncă nu există evaluări
- Depository Receipts: Presented By-Vikash Sharma (51) Ruchi BangaDocument12 paginiDepository Receipts: Presented By-Vikash Sharma (51) Ruchi Bangasuraj kumar0% (1)
- Kinship Extremes in "Desiree's BabyDocument2 paginiKinship Extremes in "Desiree's BabyĐỗ Quỳnh TrangÎncă nu există evaluări
- 20764C ENU Companion PDFDocument192 pagini20764C ENU Companion PDFAllan InurretaÎncă nu există evaluări
- Sidak 2008 FAQsDocument3 paginiSidak 2008 FAQssikhswimÎncă nu există evaluări
- Pilar Fradin ResumeDocument3 paginiPilar Fradin Resumeapi-307965130Încă nu există evaluări
- Creating A Seasonal Greeting Card RubricDocument3 paginiCreating A Seasonal Greeting Card Rubricapi-244997750Încă nu există evaluări
- Allosteric EnzymeDocument22 paginiAllosteric EnzymeAhmed ImranÎncă nu există evaluări
- Xerox 6030 PDFDocument663 paginiXerox 6030 PDFРумен ИвановÎncă nu există evaluări
- Frawley David - Wisdom of The Ancient Seers Mantras of The Rig VedaDocument140 paginiFrawley David - Wisdom of The Ancient Seers Mantras of The Rig Vedadbbircs100% (1)
- Recovering Mind and Body (Mental Health)Document24 paginiRecovering Mind and Body (Mental Health)Shivamani143100% (1)
- LP Direct & Indirect SpeechDocument7 paginiLP Direct & Indirect SpeechJoana JoaquinÎncă nu există evaluări
- 6710 NotesDocument45 pagini6710 NotesAndrés SuquilloÎncă nu există evaluări
- Garcia vs. J. Drilon G. R. No. 179267 Case DigestDocument5 paginiGarcia vs. J. Drilon G. R. No. 179267 Case DigestJoannMarieBrenda delaGenteÎncă nu există evaluări
- Introduction To Pharmacy ManagementDocument28 paginiIntroduction To Pharmacy ManagementSirry HidayaniÎncă nu există evaluări
- 7 Cancer Immunotherapy Etc-2020Document32 pagini7 Cancer Immunotherapy Etc-2020Syifa KhairunnisaÎncă nu există evaluări
- Autonomy Vs IntegrationDocument31 paginiAutonomy Vs IntegrationWahid KhanÎncă nu există evaluări
- ICTMS 2013 - Program ScheduleDocument3 paginiICTMS 2013 - Program ScheduleSantanu DasÎncă nu există evaluări
- Logic and Its Metatheory: Instructor InformationDocument6 paginiLogic and Its Metatheory: Instructor InformationMarco StoroniMazzolani Di MaioÎncă nu există evaluări
- Chong Co Thai Restaurant LocationsDocument19 paginiChong Co Thai Restaurant LocationsrajragavendraÎncă nu există evaluări
- Shamanhood and Mythology: Archaic Techniques of Ecstasy and Current Techniques of ResearchDocument22 paginiShamanhood and Mythology: Archaic Techniques of Ecstasy and Current Techniques of ResearchDunja Chrysina ChrysargyreaÎncă nu există evaluări
- 03.KUNCI KODING 11 IPA-IPS SMT 2 K13 REVISI - TP 23-24 - B.InggrisDocument2 pagini03.KUNCI KODING 11 IPA-IPS SMT 2 K13 REVISI - TP 23-24 - B.InggrisfencenbolonÎncă nu există evaluări
- Planetary MotionDocument7 paginiPlanetary Motionsuhas048Încă nu există evaluări
- 9 Oet Reading Summary 2.0-195-213Document19 pagini9 Oet Reading Summary 2.0-195-213Vijayalakshmi Narayanaswami0% (1)
- Grade 5 DLL SCIENCE 5 Q4 Week 9Document6 paginiGrade 5 DLL SCIENCE 5 Q4 Week 9Joanna Marie Cruz FelipeÎncă nu există evaluări
- Assignment 1Document2 paginiAssignment 1lauraÎncă nu există evaluări
- QP ScriptDocument57 paginiQP ScriptRitesh SharmaÎncă nu există evaluări
- Bailable and Non BailableDocument10 paginiBailable and Non BailableasthaÎncă nu există evaluări
- Activity SheetmagnetismDocument8 paginiActivity SheetmagnetismLey F. Fajutagana100% (1)