S-ar putea să vă placă și
- Laproscopic SurgeryDocument80 paginiLaproscopic SurgeryAqeel AhmadÎncă nu există evaluări
- Cardiogenic ShockDocument27 paginiCardiogenic ShockMuhammad Ikbar100% (1)
- Update in Stroke Management: David Lee Gordon, M.D., FAHADocument43 paginiUpdate in Stroke Management: David Lee Gordon, M.D., FAHAMuhidin AeÎncă nu există evaluări
- Acute Renal FailureDocument14 paginiAcute Renal FailuredrthanallaÎncă nu există evaluări
- Acute Renal Failure in The ICU PulmCritDocument27 paginiAcute Renal Failure in The ICU PulmCritchadchimaÎncă nu există evaluări
- Cardiogenic ShockDocument27 paginiCardiogenic ShockIgor StefanetÎncă nu există evaluări
- Farmakoterapi Terapan Program Pendidikan Profesi Apoteker Medan 2011Document55 paginiFarmakoterapi Terapan Program Pendidikan Profesi Apoteker Medan 2011Ika Fitri RamadhanaÎncă nu există evaluări
- Resuscitation and Shock: LSU Medical Student Clerkship, New Orleans, LADocument40 paginiResuscitation and Shock: LSU Medical Student Clerkship, New Orleans, LAFarazÎncă nu există evaluări
- Hemodynamic MonitoringDocument89 paginiHemodynamic MonitoringNia HndynÎncă nu există evaluări
- 6868841Document35 pagini6868841malik003Încă nu există evaluări
- ShockDocument2 paginiShockKemal TaufikÎncă nu există evaluări
- Cardiac Content WyattDocument90 paginiCardiac Content WyattAnni BarbaÎncă nu există evaluări
- Aki NotesDocument10 paginiAki NotesGennel Mae GarovilloÎncă nu există evaluări
- Post Op Care PH Yogya-Ok - SipDocument29 paginiPost Op Care PH Yogya-Ok - SipTaufik KurniawanÎncă nu există evaluări
- Advanced Haemodynamic MonitoringDocument29 paginiAdvanced Haemodynamic MonitoringParvathy R NairÎncă nu există evaluări
- Congestive Heart Failure, Pulmonary Edema, and CPAPDocument35 paginiCongestive Heart Failure, Pulmonary Edema, and CPAPSherwan R Shal100% (1)
- Care of Clients With Problems in Oxygenation (Part 2)Document88 paginiCare of Clients With Problems in Oxygenation (Part 2)mikErlhÎncă nu există evaluări
- My Own Critical Care NotesDocument4 paginiMy Own Critical Care NotesSamer GobreialÎncă nu există evaluări
- CHF CpapDocument35 paginiCHF CpaprahmatÎncă nu există evaluări
- GI BleedingDocument16 paginiGI BleedingWahyudinÎncă nu există evaluări
- Hemodynamic Monitoring: Martha Richter, MSN, CRNADocument89 paginiHemodynamic Monitoring: Martha Richter, MSN, CRNAners_strÎncă nu există evaluări
- Abdominal Aortic Aneurysms-EditDocument32 paginiAbdominal Aortic Aneurysms-EditrandikaÎncă nu există evaluări
- Dr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalDocument81 paginiDr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalvaishnaviÎncă nu există evaluări
- Acute Kidney InjuryDocument3 paginiAcute Kidney InjuryHarkirat AtwalÎncă nu există evaluări
- Shock: Rahayu Setyowati Bachelor of Nursing, Padjadjaran University IndonesiaDocument35 paginiShock: Rahayu Setyowati Bachelor of Nursing, Padjadjaran University IndonesiazafranÎncă nu există evaluări
- 5.2 DR - Yusuf Assegaf SPJP - Syok KardiogenikDocument33 pagini5.2 DR - Yusuf Assegaf SPJP - Syok KardiogenikAfdol Triatmojo SikumbangÎncă nu există evaluări
- Shock KGD SMT 7 PDFDocument86 paginiShock KGD SMT 7 PDFTikuqNyukUnyukUnyukÎncă nu există evaluări
- Manajemen Anestesi Pada Uremic SyndromeDocument27 paginiManajemen Anestesi Pada Uremic SyndromeAdi Nugroho MelyanaÎncă nu există evaluări
- Acute Kidney Injury: DR Hodan Ahmed Dept of Pediatrics and Child Health Amoud Medical School, AUDocument32 paginiAcute Kidney Injury: DR Hodan Ahmed Dept of Pediatrics and Child Health Amoud Medical School, AUMohamoud MohamedÎncă nu există evaluări
- Uzma Mehdi, M.D, Ms NephrologyDocument46 paginiUzma Mehdi, M.D, Ms Nephrologykrish vjÎncă nu există evaluări
- Di, Siadh, CSW Tabel PerbedaanDocument17 paginiDi, Siadh, CSW Tabel PerbedaanMichael Tambunan100% (1)
- Mechanical Ventilation AulaDocument47 paginiMechanical Ventilation Aulaapi-3820606100% (1)
- Anesthesia For Neurosurg2Document42 paginiAnesthesia For Neurosurg2Praveen RamasamyÎncă nu există evaluări
- NIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDocument38 paginiNIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDr mahi sÎncă nu există evaluări
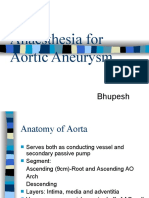
- Anaesthesia For Aortic Aneurysm: BhupeshDocument70 paginiAnaesthesia For Aortic Aneurysm: BhupeshParvathy R NairÎncă nu există evaluări
- Perioperative Acute Kidney Injury: DR Mukul Kapoor Director Anesthesia, Max Smart Super Specialty Hospital, Saket, DelhiDocument46 paginiPerioperative Acute Kidney Injury: DR Mukul Kapoor Director Anesthesia, Max Smart Super Specialty Hospital, Saket, DelhiChiragÎncă nu există evaluări
- Di, Siadh, CSWDocument17 paginiDi, Siadh, CSWNyomanGinaHennyKristiantiÎncă nu există evaluări
- Newss 2018 Hipercci - 1 PDFDocument93 paginiNewss 2018 Hipercci - 1 PDFDesyPusporiniSevenfoldismÎncă nu există evaluări
- Diagnosis & Management of Shock: W.F. Holdefer, M.D. Department of Emergency MedicineDocument27 paginiDiagnosis & Management of Shock: W.F. Holdefer, M.D. Department of Emergency MedicineCendy AndestriaÎncă nu există evaluări
- Ca ChannelDocument30 paginiCa ChannelKency DoneyÎncă nu există evaluări
- Congestive Heart FailureDocument6 paginiCongestive Heart Failureseigelystic100% (1)
- Mia Treatment Guidelines 2007Document39 paginiMia Treatment Guidelines 2007楊將群Încă nu există evaluări
- ACLS Class Packet PDFDocument9 paginiACLS Class Packet PDFImam GultomÎncă nu există evaluări
- Cardiogenic ShokDocument17 paginiCardiogenic ShokMuhammad Yasdar BahriÎncă nu există evaluări
- CPG - Acute Pulmonary Oedema - CopieDocument4 paginiCPG - Acute Pulmonary Oedema - CopieAnaid FourevaÎncă nu există evaluări
- Neonatal Hypertension: Marifi de Jesus U. Cabaluna, MDDocument61 paginiNeonatal Hypertension: Marifi de Jesus U. Cabaluna, MDJavier Casanovas LaxÎncă nu există evaluări
- CCCCCCCCCCCCCCCCCCCCC CC C C C C C C C C C C C C C C C CDocument5 paginiCCCCCCCCCCCCCCCCCCCCC CC C C C C C C C C C C C C C C C CAnn-Jillian DaangÎncă nu există evaluări
- Basics Mechanical VentilationDocument51 paginiBasics Mechanical VentilationademÎncă nu există evaluări
- Cardiogenic Shock - SWDocument41 paginiCardiogenic Shock - SWAyu LuthfiyahÎncă nu există evaluări
- Anesthesia For Emergency SurgeryDocument85 paginiAnesthesia For Emergency Surgeryansuh22100% (11)
- Albumin in Liver Cirrhosis, SADocument37 paginiAlbumin in Liver Cirrhosis, SADwinita ViviantiÎncă nu există evaluări
- Sample Medical Guidelines: ACLS-BradycardiaDocument2 paginiSample Medical Guidelines: ACLS-BradycardiaCheewin KhawprapaÎncă nu există evaluări
- Anti Aritmia IjoDocument24 paginiAnti Aritmia IjoDedy SantosoÎncă nu există evaluări
- Slide Critical CareDocument30 paginiSlide Critical Careandirio7486Încă nu există evaluări
- Lab ValuesDocument6 paginiLab ValuesdnllkzaÎncă nu există evaluări
- Acute Surgical Topics: An Infographic GuideDe la EverandAcute Surgical Topics: An Infographic GuideÎncă nu există evaluări
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideDe la EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideÎncă nu există evaluări
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosDe la EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosÎncă nu există evaluări
- What Is The Optimum Time To Start Antiretroviral Therapy in People With HIV and Tuberculosis Coinfection? A Systematic Review and Meta-AnalysisDocument34 paginiWhat Is The Optimum Time To Start Antiretroviral Therapy in People With HIV and Tuberculosis Coinfection? A Systematic Review and Meta-Analysisbagir_dm10Încă nu există evaluări
- Bartter-Like Syndrome in A Patient Receiving CapreDocument6 paginiBartter-Like Syndrome in A Patient Receiving Caprebagir_dm10Încă nu există evaluări
- Pharmacology of Echinocandins - UpToDateDocument16 paginiPharmacology of Echinocandins - UpToDatebagir_dm10Încă nu există evaluări
- Portal Hypertensive Gastropathy - UpToDateDocument27 paginiPortal Hypertensive Gastropathy - UpToDatebagir_dm10Încă nu există evaluări
- Management of Candidemia and Invasive Candidiasis in Adults - UpToDateDocument32 paginiManagement of Candidemia and Invasive Candidiasis in Adults - UpToDatebagir_dm10Încă nu există evaluări
- Reviews: Management of Hyperkalaemia in Chronic Kidney DiseaseDocument10 paginiReviews: Management of Hyperkalaemia in Chronic Kidney Diseasebagir_dm10Încă nu există evaluări
- Update CoccidioidomycosisDocument15 paginiUpdate Coccidioidomycosisbagir_dm10Încă nu există evaluări
- Overview of Autoimmune Hepatitis - UpToDateDocument33 paginiOverview of Autoimmune Hepatitis - UpToDatebagir_dm10Încă nu există evaluări
- IPD - ALF & Abses LiverDocument49 paginiIPD - ALF & Abses Liverbagir_dm10Încă nu există evaluări
- Hepatitis C Virus TreatmentDocument80 paginiHepatitis C Virus TreatmentAdrian AprotosoaieÎncă nu există evaluări
- Biology of Candida Infections - UpToDateDocument25 paginiBiology of Candida Infections - UpToDatebagir_dm10Încă nu există evaluări
- 12 Internal BleedingDocument40 pagini12 Internal BleedingNoval LiadyÎncă nu există evaluări
- IPD - ALF & Abses LiverDocument49 paginiIPD - ALF & Abses Liverbagir_dm10Încă nu există evaluări
- BM 3 & 4 - Replikasi, Transkripsi, Translasi (Prof Indri)Document61 paginiBM 3 & 4 - Replikasi, Transkripsi, Translasi (Prof Indri)bagir_dm10Încă nu există evaluări
- Ventricular Tachycardia - Budi Baktijasa, MD, FIHA PDFDocument33 paginiVentricular Tachycardia - Budi Baktijasa, MD, FIHA PDFbagir_dm10Încă nu există evaluări
- Multiple Mieloma-1Document3 paginiMultiple Mieloma-1bagir_dm10Încă nu există evaluări
- Acute Limb Ischemia - J. Nugroho Eko, MD, PHD, FIHA PDFDocument31 paginiAcute Limb Ischemia - J. Nugroho Eko, MD, PHD, FIHA PDFbagir_dm10Încă nu există evaluări
- STEMI - I Gde Rurus Suryawan, MD, FIHA PDFDocument33 paginiSTEMI - I Gde Rurus Suryawan, MD, FIHA PDFbagir_dm10100% (1)
- DR - Lefi Lunch Sympo PDFDocument30 paginiDR - Lefi Lunch Sympo PDFbagir_dm10Încă nu există evaluări
- Practical Neurology PDFDocument771 paginiPractical Neurology PDFCurtali Licdan100% (3)
- Unstable Angina - NSTEMI - Muhammad Aminuddin, MD, FIHA PDFDocument39 paginiUnstable Angina - NSTEMI - Muhammad Aminuddin, MD, FIHA PDFbagir_dm10Încă nu există evaluări
- Supraventricular Tachycardia - Achmad Lefi, MD, FIHA PDFDocument38 paginiSupraventricular Tachycardia - Achmad Lefi, MD, FIHA PDFbagir_dm10Încă nu există evaluări
- Pulmonary Embolism - Iswanto Pratanu, MD, FIHA PDFDocument30 paginiPulmonary Embolism - Iswanto Pratanu, MD, FIHA PDFbagir_dm10Încă nu există evaluări
- Post Resuscitation Syndrome - Andrianto, MD, FIHA PDFDocument33 paginiPost Resuscitation Syndrome - Andrianto, MD, FIHA PDFbagir_dm10Încă nu există evaluări
- DR - Saifur Prelunch Sympo PDFDocument37 paginiDR - Saifur Prelunch Sympo PDFbagir_dm10Încă nu există evaluări
- DR - Iswanto Sympo-3 PDFDocument29 paginiDR - Iswanto Sympo-3 PDFbagir_dm10Încă nu există evaluări
- Prof - Djoko Prelunch Sympo PDFDocument43 paginiProf - Djoko Prelunch Sympo PDFbagir_dm10Încă nu există evaluări
- Prof Djoko Plenary PDFDocument23 paginiProf Djoko Plenary PDFbagir_dm10Încă nu există evaluări
- Management of Bleeding Due To Antithrombotic - Soeharsohadi, MD, FIHA PDFDocument28 paginiManagement of Bleeding Due To Antithrombotic - Soeharsohadi, MD, FIHA PDFbagir_dm10Încă nu există evaluări
- DR - Nugroho Lunch Sympo PDFDocument26 paginiDR - Nugroho Lunch Sympo PDFbagir_dm10Încă nu există evaluări
- BirdLife South Africa Checklist of Birds 2023 ExcelDocument96 paginiBirdLife South Africa Checklist of Birds 2023 ExcelAkash AnandrajÎncă nu există evaluări
- Polymeric Nanoparticles - Recent Development in Synthesis and Application-2016Document19 paginiPolymeric Nanoparticles - Recent Development in Synthesis and Application-2016alex robayoÎncă nu există evaluări
- Togaf Open Group Business ScenarioDocument40 paginiTogaf Open Group Business Scenariohmh97Încă nu există evaluări
- Design of Corn ThresherDocument11 paginiDesign of Corn ThresherFrancisco ToroÎncă nu există evaluări
- (Methods in Molecular Biology 1496) William J. Brown - The Golgi Complex - Methods and Protocols-Humana Press (2016)Document233 pagini(Methods in Molecular Biology 1496) William J. Brown - The Golgi Complex - Methods and Protocols-Humana Press (2016)monomonkisidaÎncă nu există evaluări
- DMemo For Project RBBDocument28 paginiDMemo For Project RBBRiza Guste50% (8)
- FIREXDocument2 paginiFIREXPausÎncă nu există evaluări
- 37 Sample Resolutions Very Useful, Indian Companies Act, 1956Document38 pagini37 Sample Resolutions Very Useful, Indian Companies Act, 1956CA Vaibhav Maheshwari70% (23)
- Employer'S Virtual Pag-Ibig Enrollment Form: Address and Contact DetailsDocument2 paginiEmployer'S Virtual Pag-Ibig Enrollment Form: Address and Contact DetailstheffÎncă nu există evaluări
- Malate SynthaseDocument8 paginiMalate SynthaseMinichÎncă nu există evaluări
- Discrete Probability Distribution UpdatedDocument44 paginiDiscrete Probability Distribution UpdatedWaylonÎncă nu există evaluări
- PT - Science 5 - Q1Document4 paginiPT - Science 5 - Q1Jomelyn MaderaÎncă nu există evaluări
- 9francisco Gutierrez Et Al. v. Juan CarpioDocument4 pagini9francisco Gutierrez Et Al. v. Juan Carpiosensya na pogi langÎncă nu există evaluări
- APICS-Houston Newsletter Sept 2012Document16 paginiAPICS-Houston Newsletter Sept 2012Christopher SeifertÎncă nu există evaluări
- Thomas Noochan Pokemon Review Final DraftDocument6 paginiThomas Noochan Pokemon Review Final Draftapi-608717016Încă nu există evaluări
- Final ReflectionDocument4 paginiFinal Reflectionapi-314231777Încă nu există evaluări
- Gamboa Vs Chan 2012 Case DigestDocument2 paginiGamboa Vs Chan 2012 Case DigestKrissa Jennesca Tullo100% (2)
- La Fonction Compositionnelle Des Modulateurs en Anneau Dans: MantraDocument6 paginiLa Fonction Compositionnelle Des Modulateurs en Anneau Dans: MantracmescogenÎncă nu există evaluări
- K3VG Spare Parts ListDocument1 paginăK3VG Spare Parts ListMohammed AlryaniÎncă nu există evaluări
- Final Module in Human BehaviorDocument60 paginiFinal Module in Human BehaviorNarag Krizza50% (2)
- Pediatric ECG Survival Guide - 2nd - May 2019Document27 paginiPediatric ECG Survival Guide - 2nd - May 2019Marcos Chusin MontesdeocaÎncă nu există evaluări
- Flabbergasted! - Core RulebookDocument160 paginiFlabbergasted! - Core RulebookRobert RichesonÎncă nu există evaluări
- Speaking Test FeedbackDocument12 paginiSpeaking Test FeedbackKhong TrangÎncă nu există evaluări
- SQ1 Mogas95Document1 paginăSQ1 Mogas95Basant Kumar SaxenaÎncă nu există evaluări
- Gee 103 L3 Ay 22 23 PDFDocument34 paginiGee 103 L3 Ay 22 23 PDFlhyka nogalesÎncă nu există evaluări
- PEG Catalog Siemens PDFDocument419 paginiPEG Catalog Siemens PDFrukmagoudÎncă nu există evaluări
- Church A Rchitecture Abbey: Throne" Ecclesia Cathedralis (In Latin)Document18 paginiChurch A Rchitecture Abbey: Throne" Ecclesia Cathedralis (In Latin)Pat GeronzÎncă nu există evaluări
- RESO NO. 4 - LANYARD FinalDocument1 paginăRESO NO. 4 - LANYARD FinalsharonleefulloÎncă nu există evaluări
- Test AmeeshDocument7 paginiTest AmeeshUdit DravidÎncă nu există evaluări
- Answers To Quiz No 19Document5 paginiAnswers To Quiz No 19Your Public Profile100% (4)