S-ar putea să vă placă și
- Mkasap Endocrinology NotesDocument6 paginiMkasap Endocrinology NotesUm HamoOdÎncă nu există evaluări
- Asbestos, Asbestosis and Cáncer. Helsinski Critera For Diagnosis and Attribution2014 para - WebDocument155 paginiAsbestos, Asbestosis and Cáncer. Helsinski Critera For Diagnosis and Attribution2014 para - Webmarec100% (1)
- Pregnancy TestDocument10 paginiPregnancy TestquerokeropiÎncă nu există evaluări
- Pebc TextbooksDocument3 paginiPebc TextbooksJhun0% (1)
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsDe la EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsÎncă nu există evaluări
- Portal HypertensionDocument65 paginiPortal HypertensionVenu MadhavÎncă nu există evaluări
- Abdominal Surgical Emergencies in Infants and Young ChildrenDocument27 paginiAbdominal Surgical Emergencies in Infants and Young ChildrenBrenda CaraveoÎncă nu există evaluări
- AscitesDocument36 paginiAscitesmiki0% (1)
- RH IncompatibilityDocument22 paginiRH IncompatibilityDrPreeti Thakur ChouhanÎncă nu există evaluări
- Abdominal Sweliing and AscitesDocument72 paginiAbdominal Sweliing and AscitesFernando Aniban100% (1)
- Portal Vein Thrombosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandPortal Vein Thrombosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Hepatorenal Syndrome: Causes, Tests, and Treatment OptionsDe la EverandHepatorenal Syndrome: Causes, Tests, and Treatment OptionsEvaluare: 4.5 din 5 stele4.5/5 (2)
- Cirrhosis of LiverDocument22 paginiCirrhosis of LiverKrini Tandel50% (2)
- Rectal Cancer Contouring Guide: Econtour TeamDocument29 paginiRectal Cancer Contouring Guide: Econtour TeamRonna Marie Vijar PamalandongÎncă nu există evaluări
- Presented By: Medicine Unit 1Document95 paginiPresented By: Medicine Unit 1Abdullah Muceddidi100% (1)
- Pa Tho Physiology of Liver Cirrhosis - MercyDocument7 paginiPa Tho Physiology of Liver Cirrhosis - Mercymersenie_TheovercomerÎncă nu există evaluări
- Nursing Republic Acts - PhilippinesDocument2 paginiNursing Republic Acts - PhilippinesLj Ferolino100% (11)
- Ascites in ChildrenDocument7 paginiAscites in Childrentriska antonyÎncă nu există evaluări
- JURNAL Ascites PDFDocument9 paginiJURNAL Ascites PDFican_parlenteÎncă nu există evaluări
- Ascitis PDFDocument17 paginiAscitis PDFLeonardo MagónÎncă nu există evaluări
- AscitesascitesDocument15 paginiAscitesascitesKevinJuliusTanadyÎncă nu există evaluări
- Canine AscitesDocument7 paginiCanine AscitesGabriel Coelho GimenesÎncă nu există evaluări
- Ascitis ImportanteDocument17 paginiAscitis Importantedanyescalerapumas24Încă nu există evaluări
- Ascites: Peritoneal Cavity MedicalDocument4 paginiAscites: Peritoneal Cavity MedicalVenkatesan VidhyaÎncă nu există evaluări
- Jurnal Ascites PDFDocument8 paginiJurnal Ascites PDFYunia DwiÎncă nu există evaluări
- AscitesDocument5 paginiAscitesEeshuAomÎncă nu există evaluări
- Ascietes by DR Naila MasoodDocument45 paginiAscietes by DR Naila MasoodmichelleÎncă nu există evaluări
- Aasld 2021 Ascite, Pbe e SHR PDFDocument77 paginiAasld 2021 Ascite, Pbe e SHR PDFAna ClaudiaÎncă nu există evaluări
- Major Complication of CirrhosisDocument6 paginiMajor Complication of CirrhosisAlya Putri KhairaniÎncă nu există evaluări
- The Diagnostic Work-Up in Patients With Ascites Current Guidelines and Future ProspectsDocument6 paginiThe Diagnostic Work-Up in Patients With Ascites Current Guidelines and Future ProspectsCAMILO FERRERO RESTREPOÎncă nu există evaluări
- The Diagnostic Work-Up in Patients With Ascites: Current Guidelines and Future ProspectsDocument7 paginiThe Diagnostic Work-Up in Patients With Ascites: Current Guidelines and Future ProspectsRizqi AmaliaÎncă nu există evaluări
- Ascites: Phillip S. Ge, MD, Carlos Guarner, MD, PHD, and Bruce A. Runyon, MDDocument12 paginiAscites: Phillip S. Ge, MD, Carlos Guarner, MD, PHD, and Bruce A. Runyon, MDTere DelgadoÎncă nu există evaluări
- Gastrointestinal Bleeding and ManagementDocument19 paginiGastrointestinal Bleeding and ManagementMarcela HincapiéÎncă nu există evaluări
- Sirrhosis HatiDocument6 paginiSirrhosis HatikimokberusungÎncă nu există evaluări
- Extrahepatic Biliary AtresiaDocument3 paginiExtrahepatic Biliary AtresiaTiti Afrianto100% (1)
- Cirrhosis of LiverDocument6 paginiCirrhosis of LiverpakdejackÎncă nu există evaluări
- Esophageal VaricesDocument12 paginiEsophageal VaricesgemergencycareÎncă nu există evaluări
- Help Pedsurgeryafrica80Document4 paginiHelp Pedsurgeryafrica80Thayalan SukumaranÎncă nu există evaluări
- B.SC Nursing Medical Surgical Nursing - I Unit: Iv - Nursing Management of Patients With Disorders of Digestive System Portal HypertensionDocument32 paginiB.SC Nursing Medical Surgical Nursing - I Unit: Iv - Nursing Management of Patients With Disorders of Digestive System Portal HypertensionPoova RagavanÎncă nu există evaluări
- Portal HypertensionDocument13 paginiPortal HypertensionCiprian BoesanÎncă nu există evaluări
- Chronic Liver FailureDocument4 paginiChronic Liver FailureJasmine Faith SilvaÎncă nu există evaluări
- Jasmin O. Dingle BSN-4y1-3CDocument6 paginiJasmin O. Dingle BSN-4y1-3CJasmn DingleÎncă nu există evaluări
- Neonatal CholestasisDocument5 paginiNeonatal CholestasisMateen ShukriÎncă nu există evaluări
- Approach To The Jaundiced Cat - WSAVA 2015 Congress - VINDocument6 paginiApproach To The Jaundiced Cat - WSAVA 2015 Congress - VINdmantsioÎncă nu există evaluări
- Ed Ascites PDFDocument47 paginiEd Ascites PDFradicalmpÎncă nu există evaluări
- Hepatic Cirrhosis and Hepatitis: Dr. Lubna DwerijDocument69 paginiHepatic Cirrhosis and Hepatitis: Dr. Lubna DwerijNoor MajaliÎncă nu există evaluări
- Pathohysiology of Ascites: Waleed Al-HamoudiDocument36 paginiPathohysiology of Ascites: Waleed Al-Hamoudiarina31Încă nu există evaluări
- Urinary Tract DisordersDocument54 paginiUrinary Tract Disorderssharon ocharaÎncă nu există evaluări
- Management of End-Stage Liver DiseaseDocument34 paginiManagement of End-Stage Liver DiseaseAldo IbarraÎncă nu există evaluări
- Esophageal VaricesDocument9 paginiEsophageal VaricesErina WahyuniÎncă nu există evaluări
- Liver Cirrhis Due To Upper Gi BleedingDocument5 paginiLiver Cirrhis Due To Upper Gi BleedingNathaniel BudayÎncă nu există evaluări
- Approach To Upper Gastrointestinal Bleeding in Children PDFDocument13 paginiApproach To Upper Gastrointestinal Bleeding in Children PDFandreita1741Încă nu există evaluări
- NCM Lecture (Liver and Gallbladder)Document76 paginiNCM Lecture (Liver and Gallbladder)beer_ettaaÎncă nu există evaluări
- AscitesDocument71 paginiAscitessohilaw210Încă nu există evaluări
- Abdominal Swelling: Ela-BelaDocument48 paginiAbdominal Swelling: Ela-BelaHassen Kavi IsseÎncă nu există evaluări
- NCP CKD From CaneDocument74 paginiNCP CKD From CaneSheela Khrystyn LeeÎncă nu există evaluări
- Journal Of: Gastroenterology and Hepatology ResearchDocument7 paginiJournal Of: Gastroenterology and Hepatology ResearchparkfishyÎncă nu există evaluări
- Gambaran Angka Kejadian, Karakteristik Dan Ekspertise Radiologi USG Pasien Asites Di RS Al-Ihsan Periode 2013-2015Document6 paginiGambaran Angka Kejadian, Karakteristik Dan Ekspertise Radiologi USG Pasien Asites Di RS Al-Ihsan Periode 2013-2015Ria Rizki JayantiÎncă nu există evaluări
- Progesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichDocument9 paginiProgesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichFerreze AnnÎncă nu există evaluări
- Progesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichDocument9 paginiProgesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichFerreze AnnÎncă nu există evaluări
- Biliary Atresia TeoriDocument22 paginiBiliary Atresia TeoriHudza RabbaniÎncă nu există evaluări
- Evaluation of Adults With AscitesDocument16 paginiEvaluation of Adults With AscitesMaricruz BracamonteÎncă nu există evaluări
- Paracentesis: Analysate InterpretationDocument2 paginiParacentesis: Analysate InterpretationNor Ubudiah SetiÎncă nu există evaluări
- Ascites Full TopicDocument15 paginiAscites Full TopicAashiÎncă nu există evaluări
- Lecture On Conjugated HyperbilirubinaemiaDocument38 paginiLecture On Conjugated HyperbilirubinaemiaIgwe SolomonÎncă nu există evaluări
- Uworld GI NotesDocument17 paginiUworld GI NotesAyodeji SotimehinÎncă nu există evaluări
- Help Pedsurgeryafrica81Document7 paginiHelp Pedsurgeryafrica81tikaauliaÎncă nu există evaluări
- Clinical Manifestations and Diagnosis of Urinary Tract Obstruction and Hydroneph PDFDocument32 paginiClinical Manifestations and Diagnosis of Urinary Tract Obstruction and Hydroneph PDFAmjad Saud0% (1)
- Plaquetas en NeonatosDocument6 paginiPlaquetas en NeonatosBrenda CaraveoÎncă nu există evaluări
- c1q NefropatiaDocument6 paginic1q NefropatiaBrenda CaraveoÎncă nu există evaluări
- Isolation 2007Document225 paginiIsolation 2007Kiageng NicoÎncă nu există evaluări
- Mucositis PatobiologiaDocument9 paginiMucositis PatobiologiaBrenda CaraveoÎncă nu există evaluări
- Cerebral EdemaDocument6 paginiCerebral EdemaantonopoulosalÎncă nu există evaluări
- Hypercholesterolemia Among Children: When Is It High, and When Is It Really High?Document4 paginiHypercholesterolemia Among Children: When Is It High, and When Is It Really High?Brenda CaraveoÎncă nu există evaluări
- Probioticos en DiarreaDocument126 paginiProbioticos en DiarreaBrenda CaraveoÎncă nu există evaluări
- BackpainDocument10 paginiBackpainBrenda CaraveoÎncă nu există evaluări
- Anemia MicrociticaDocument15 paginiAnemia MicrociticaBrenda CaraveoÎncă nu există evaluări
- Treatment of Allergic Rhinitis PDFDocument23 paginiTreatment of Allergic Rhinitis PDFLydia MamurÎncă nu există evaluări
- ARIAReport 2010Document153 paginiARIAReport 2010Syairah Banu DjufriÎncă nu există evaluări
- Absceso Cerebral 99Document7 paginiAbsceso Cerebral 99shen_siiÎncă nu există evaluări
- KawasakiDocument11 paginiKawasakiBrenda CaraveoÎncă nu există evaluări
- Alimentacionen Circunstancias EspecialesDocument9 paginiAlimentacionen Circunstancias EspecialesBrenda CaraveoÎncă nu există evaluări
- 22Q11.2 Distal Deletion: A Recurrent Genomic Disorder Distinct From Digeorge Syndrome and Velocardiofacial SyndromeDocument8 pagini22Q11.2 Distal Deletion: A Recurrent Genomic Disorder Distinct From Digeorge Syndrome and Velocardiofacial SyndromeBrenda CaraveoÎncă nu există evaluări
- Diagnostic Approach and Management of Cow S Milk.28Document9 paginiDiagnostic Approach and Management of Cow S Milk.28minerva_stanciuÎncă nu există evaluări
- Cerebral Palsy - RomantsevaDocument13 paginiCerebral Palsy - RomantsevaBrenda CaraveoÎncă nu există evaluări
- Trombocitopenia Inmune PrimariaDocument13 paginiTrombocitopenia Inmune PrimariaBrenda CaraveoÎncă nu există evaluări
- Cerebral Palsy - RomantsevaDocument13 paginiCerebral Palsy - RomantsevaBrenda CaraveoÎncă nu există evaluări
- AnafilaxisDocument11 paginiAnafilaxisJoãoBrasilÎncă nu există evaluări
- Adenomegalias 08Document10 paginiAdenomegalias 08Brenda CaraveoÎncă nu există evaluări
- Diagnosis and Treatment of Atopic DermatitisDocument19 paginiDiagnosis and Treatment of Atopic DermatitisBrenda CaraveoÎncă nu există evaluări
- Antibiticoterapia en Sepsis Tardia NeoreviewsDocument11 paginiAntibiticoterapia en Sepsis Tardia NeoreviewsBrenda CaraveoÎncă nu există evaluări
- Acidosis y AlcalosisDocument10 paginiAcidosis y AlcalosisBrenda CaraveoÎncă nu există evaluări
- Alt Coagulacion 08Document12 paginiAlt Coagulacion 08Brenda CaraveoÎncă nu există evaluări
- Hypo Thyroid Is Mped in ReviewDocument10 paginiHypo Thyroid Is Mped in ReviewBrenda CaraveoÎncă nu există evaluări
- Update On Food AllergyDocument15 paginiUpdate On Food AllergyBrenda CaraveoÎncă nu există evaluări
- Respiratory Manifestations of Food AllergyDocument8 paginiRespiratory Manifestations of Food AllergyBrenda CaraveoÎncă nu există evaluări
- Case Presentation: EclampsiaDocument44 paginiCase Presentation: Eclampsiamutiara sitepuÎncă nu există evaluări
- Maternal SepsisDocument50 paginiMaternal SepsisMahmoud Abu Al AmrainÎncă nu există evaluări
- Morton's Metatarsalgia - Pathogenesis, Aetiology and Current ManagementDocument10 paginiMorton's Metatarsalgia - Pathogenesis, Aetiology and Current ManagementLikhit NayakÎncă nu există evaluări
- Case Pres ZandiOrstDocument17 paginiCase Pres ZandiOrstNajeeb UllahÎncă nu există evaluări
- Faktor Determinan Psikososial Dan Mediko Obstetrik Pada Pasien InggrisDocument15 paginiFaktor Determinan Psikososial Dan Mediko Obstetrik Pada Pasien Inggrisandika setionoÎncă nu există evaluări
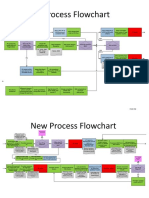
- New Process Flowchart CPOEDocument4 paginiNew Process Flowchart CPOELiza GeorgeÎncă nu există evaluări
- Flyer SugiesDocument2 paginiFlyer SugiesInomy ClaudiaÎncă nu există evaluări
- Solitaire Company ProfileDocument71 paginiSolitaire Company ProfilesolitairepharmaciaÎncă nu există evaluări
- A Brief History of Women in SurgeryDocument3 paginiA Brief History of Women in SurgeryMargarita AucejoÎncă nu există evaluări
- Esaote MyLab40 BrochureDocument8 paginiEsaote MyLab40 BrochureDiegoÎncă nu există evaluări
- Nursing in Islam: PDF Created With Pdffactory Pro Trial VersionDocument12 paginiNursing in Islam: PDF Created With Pdffactory Pro Trial VersionFarzana AfrinÎncă nu există evaluări
- Mouth Care Guideline - Final Oct 15 v1 ApprovedDocument12 paginiMouth Care Guideline - Final Oct 15 v1 ApprovedFitri Perdana PutriÎncă nu există evaluări
- Powders and CachetsDocument2 paginiPowders and CachetsVandittJhingranÎncă nu există evaluări
- Pederson PDFDocument5 paginiPederson PDFCosmina EnescuÎncă nu există evaluări
- Supersize Me EssayDocument5 paginiSupersize Me EssayBrooke Cohn0% (1)
- Diabetic Ketoacidosis in PregnancyDocument12 paginiDiabetic Ketoacidosis in PregnancyMuhammad BilalÎncă nu există evaluări
- Sedimento UrinarioDocument13 paginiSedimento UrinarioNaruto ShikamaruÎncă nu există evaluări
- Orthopaedic MasterDocument4 paginiOrthopaedic MasterMaxpain MaxÎncă nu există evaluări
- Central Line Blood DrawDocument20 paginiCentral Line Blood DrawAnonymous fDSnTnWsfGÎncă nu există evaluări
- Fcps & MRCP (UK) Career Counselling For Rifao RMU SymposiumDocument58 paginiFcps & MRCP (UK) Career Counselling For Rifao RMU SymposiumSamÎncă nu există evaluări
- VBAC ScoreDocument3 paginiVBAC ScorepraburastraÎncă nu există evaluări
- Cad Effectiveness of Smartphone-Based Mindfulness Training On Maternal Perinatal Depression Randomized Controlled TrialDocument23 paginiCad Effectiveness of Smartphone-Based Mindfulness Training On Maternal Perinatal Depression Randomized Controlled TrialZir LakedÎncă nu există evaluări
- 3 - Advances in The Diagnosis and Treatment of VasculitisDocument378 pagini3 - Advances in The Diagnosis and Treatment of VasculitisAnonymous nGhxGKWXJr100% (1)