S-ar putea să vă placă și
- Health HistoryDocument1 paginăHealth Historymolly_hayes_24Încă nu există evaluări
- Sdcep Ohar All Example Recording Forms A4Document20 paginiSdcep Ohar All Example Recording Forms A4yazanÎncă nu există evaluări
- Medical Form FillableDocument4 paginiMedical Form Fillablefrancislouisa4Încă nu există evaluări
- Blank Medical Information SheetDocument2 paginiBlank Medical Information SheetPsalm TabatÎncă nu există evaluări
- Medical FormDocument2 paginiMedical FormHoney AliÎncă nu există evaluări
- Professional Football Club Registration & Consent Form: Personal Information - Child / Young PersonDocument2 paginiProfessional Football Club Registration & Consent Form: Personal Information - Child / Young PersonanilÎncă nu există evaluări
- Student Enrollment Health Card (F-4-HSU-003)Document2 paginiStudent Enrollment Health Card (F-4-HSU-003)Gy FalcasantosÎncă nu există evaluări
- Children S Services Referral FormDocument4 paginiChildren S Services Referral FormChinggay CuarterosÎncă nu există evaluări
- Maryland Occ1215Document3 paginiMaryland Occ1215why2kliuÎncă nu există evaluări
- Med Q English PDFDocument2 paginiMed Q English PDFxryanxÎncă nu există evaluări
- Medical and Physical Exam FormDocument2 paginiMedical and Physical Exam FormkhohannahfaithÎncă nu există evaluări
- Child Adol Traditional Biopsychosocial TemplateDocument11 paginiChild Adol Traditional Biopsychosocial Templateyeney armenteros100% (1)
- HTD Youth Camp Medical and Consent FormDocument2 paginiHTD Youth Camp Medical and Consent FormChris BowditchÎncă nu există evaluări
- Medical Form & Document ChecklistDocument2 paginiMedical Form & Document Checklistrjadhav0075Încă nu există evaluări
- Medical Form 4-12 YearsDocument1 paginăMedical Form 4-12 YearsJackson SilvaÎncă nu există evaluări
- LLC Health FormDocument2 paginiLLC Health Formcesar maguigadÎncă nu există evaluări
- Application Form - Campus HiringDocument5 paginiApplication Form - Campus Hiringpawan khattarÎncă nu există evaluări
- Students Health Info Form W SealDocument1 paginăStudents Health Info Form W SealivyÎncă nu există evaluări
- Application Form - Campus HiringDocument5 paginiApplication Form - Campus HiringDhanu T AÎncă nu există evaluări
- Uqms PirDocument2 paginiUqms PirJameslÎncă nu există evaluări
- Medical Application Form: Insured Name: Inception DateDocument3 paginiMedical Application Form: Insured Name: Inception DateDidier G PeñuelaÎncă nu există evaluări
- WCM Medical FormDocument4 paginiWCM Medical Formjewel_meltonÎncă nu există evaluări
- Authorization To Consent To Treatment of A Minor 2012Document2 paginiAuthorization To Consent To Treatment of A Minor 2012Nakuru SandwichÎncă nu există evaluări
- Jamboree Form No. 01 Participants Application FormDocument2 paginiJamboree Form No. 01 Participants Application FormNELSON JR TUMALAÎncă nu există evaluări
- Emergency Contacts and Information ForDocument1 paginăEmergency Contacts and Information Forkaylynn4Încă nu există evaluări
- Electronic Health Record: Log inDocument42 paginiElectronic Health Record: Log inArian May MarcosÎncă nu există evaluări
- Brendahs Medical FormDocument2 paginiBrendahs Medical FormBaluku GeofreyÎncă nu există evaluări
- Please Complete in Full or Attach A Copy of Your Child's Vaccination Record To The FormDocument2 paginiPlease Complete in Full or Attach A Copy of Your Child's Vaccination Record To The FormRohit JÎncă nu există evaluări
- New Patient Application UpdatedDocument5 paginiNew Patient Application UpdatedAbdu AryaÎncă nu există evaluări
- Child's Details: Date of Birth: Nric/Bc/Fin: NameDocument2 paginiChild's Details: Date of Birth: Nric/Bc/Fin: NameAndy LimÎncă nu există evaluări
- Medical Form and Food Allergen FormDocument4 paginiMedical Form and Food Allergen FormacastillofuguetÎncă nu există evaluări
- Physical Form 2018Document2 paginiPhysical Form 2018api-247134277Încă nu există evaluări
- Health Declaration FormDocument3 paginiHealth Declaration FormMaja Aira BumatayÎncă nu există evaluări
- Pre Medical Form PDFDocument11 paginiPre Medical Form PDFNitin KumarÎncă nu există evaluări
- Confidential United Nations Nations Unies Employment Medical Review QuestionnaireDocument2 paginiConfidential United Nations Nations Unies Employment Medical Review QuestionnaireMartin Mambu100% (1)
- Medical History Form 3 Years and OlderDocument3 paginiMedical History Form 3 Years and OlderJalisha SarmientoÎncă nu există evaluări
- Medical Admission Proforma: Hospital Name Patient DetailsDocument11 paginiMedical Admission Proforma: Hospital Name Patient DetailsAngelus129Încă nu există evaluări
- Year 9 Camp Health and Medical ConsentDocument3 paginiYear 9 Camp Health and Medical ConsentFiona CharringtonÎncă nu există evaluări
- Australian Immunisation Register Ceasing Correspondence and Release of InformationDocument2 paginiAustralian Immunisation Register Ceasing Correspondence and Release of InformationAshlee0% (2)
- Confidential United Nations Nations Unies Employment Medical Review QuestionnaireDocument2 paginiConfidential United Nations Nations Unies Employment Medical Review QuestionnaireHaythem FarhatiÎncă nu există evaluări
- Family First Chiropractic Client Intake 03172Document6 paginiFamily First Chiropractic Client Intake 03172Trina AsterinoÎncă nu există evaluări
- Health History FormDocument3 paginiHealth History Formraysa mendezÎncă nu există evaluări
- Corporate Membership Application FormDocument2 paginiCorporate Membership Application Formpradhan13100% (1)
- Medical Application Form PDFDocument3 paginiMedical Application Form PDFHumanÎncă nu există evaluări
- Worker Health SheetDocument1 paginăWorker Health SheetScribdTranslationsÎncă nu există evaluări
- Medical Information and Permission SlipDocument1 paginăMedical Information and Permission Slipapi-238173638Încă nu există evaluări
- GreatAuPair Medical Evaluation Form 01012014Document4 paginiGreatAuPair Medical Evaluation Form 01012014EhickyyÎncă nu există evaluări
- General Patient HistoryDocument1 paginăGeneral Patient HistoryRaul LipataÎncă nu există evaluări
- Student Medical RecordDocument3 paginiStudent Medical Recordhamsa RasbiehÎncă nu există evaluări
- Medical Questionnaire Sept 06Document2 paginiMedical Questionnaire Sept 06Rein Potential Applicant100% (1)
- Day Care Registration (Blue Card)Document2 paginiDay Care Registration (Blue Card)Nikki NievesÎncă nu există evaluări
- PAR1514 Medical HistoryDocument5 paginiPAR1514 Medical Historyloxav71284Încă nu există evaluări
- Anamnesis For Dental Health CareDocument1 paginăAnamnesis For Dental Health CarePaulo CastroÎncă nu există evaluări
- Adult Standard Biopsychosocial TemplateDocument11 paginiAdult Standard Biopsychosocial Templateapi-404660807Încă nu există evaluări
- EmaSwatiCare Company Application Form 2023Document4 paginiEmaSwatiCare Company Application Form 2023jinearkayendaÎncă nu există evaluări
- Medical History FormDocument2 paginiMedical History Formapi-279870303Încă nu există evaluări
- Travel Insurance Application Form - Updated PDFDocument2 paginiTravel Insurance Application Form - Updated PDFAnonymous Nw6c3H0Încă nu există evaluări
- Turner Syndrome: Pathophysiology, Diagnosis and TreatmentDe la EverandTurner Syndrome: Pathophysiology, Diagnosis and TreatmentPatricia Y. FechnerÎncă nu există evaluări
- Parent Guardian PermissionDocument1 paginăParent Guardian PermissionHKantesÎncă nu există evaluări
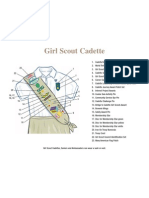
- Uniform CadetteDocument1 paginăUniform CadetteHKantesÎncă nu există evaluări
- Cheer Leading MotionsDocument2 paginiCheer Leading MotionsHKantesÎncă nu există evaluări
- Consent and WaiverDocument1 paginăConsent and WaiverHKantesÎncă nu există evaluări
- Offense and DefenseDocument1 paginăOffense and DefenseHKantesÎncă nu există evaluări
- Congratulations To SendDocument37 paginiCongratulations To SendLeslie Anne BiteÎncă nu există evaluări
- Fundamentals of NursingDocument268 paginiFundamentals of Nursinguhta100% (1)
- Perio Case HistoryDocument90 paginiPerio Case HistoryMoola Bharath ReddyÎncă nu există evaluări
- Case 10: Placenta Previa: ST ND RDDocument6 paginiCase 10: Placenta Previa: ST ND RDMengda ZhangÎncă nu există evaluări
- Canadas Food Guide Serving SizesDocument2 paginiCanadas Food Guide Serving SizesVictor EstradaÎncă nu există evaluări
- Pharmacotherapy Update in Heart Failure: Siti Elkana Nauli Tangerang District HospitalDocument45 paginiPharmacotherapy Update in Heart Failure: Siti Elkana Nauli Tangerang District HospitalFadly AminÎncă nu există evaluări
- Anaesthetic Considerations in Patients With Transverse MyelitisDocument3 paginiAnaesthetic Considerations in Patients With Transverse MyelitisIniya RajendranÎncă nu există evaluări
- Diabetic KetoacidosisDocument38 paginiDiabetic KetoacidosisAwatef AbushhiwaÎncă nu există evaluări
- Dialog Perawat Dan PerawatDocument5 paginiDialog Perawat Dan PerawatnandaÎncă nu există evaluări
- 7 Dr. Dineros - PhilHealth CHO MHODocument15 pagini7 Dr. Dineros - PhilHealth CHO MHOKristel Joy Verzon-BunaganÎncă nu există evaluări
- How The NTSB Conducts InvestigationsDocument3 paginiHow The NTSB Conducts InvestigationsVarman Aviation Quality DeptÎncă nu există evaluări
- Colorectal Cancer A ReviewDocument11 paginiColorectal Cancer A ReviewMarcelitaTaliaDuwiriÎncă nu există evaluări
- RejectedDocument2 paginiRejectedAutismeyeÎncă nu există evaluări
- Cognitive Training and Cognitive Rehabilitation For People With Early-Stage Alzheimer's Disease - Review - Clare & WoodsDocument18 paginiCognitive Training and Cognitive Rehabilitation For People With Early-Stage Alzheimer's Disease - Review - Clare & WoodsRegistro psiÎncă nu există evaluări
- Name: Ponce, Christian Neil P. Subject: CHN2 Course and Year: Bsn3 Block1. Code:N113Document3 paginiName: Ponce, Christian Neil P. Subject: CHN2 Course and Year: Bsn3 Block1. Code:N113Novelyn PuaÎncă nu există evaluări
- OET Practice Reading Test Part A:: JourneyDocument9 paginiOET Practice Reading Test Part A:: JourneyPrasoon PremrajÎncă nu există evaluări
- Jeevansathi-Compatibility Report: A Quick Look at YourDocument14 paginiJeevansathi-Compatibility Report: A Quick Look at YourNeha GirdharÎncă nu există evaluări
- Holidaybreak CS PDFDocument2 paginiHolidaybreak CS PDFandrea94Încă nu există evaluări
- BrufenDocument4 paginiBrufensofronije2005Încă nu există evaluări
- InfluenzaDocument13 paginiInfluenzaBarbara Preiss100% (2)
- Mapeh Pre PostDocument6 paginiMapeh Pre PostCathy Fern GonzalesÎncă nu există evaluări
- Hitachi Solutions - ETIQA - Application Form (Signed)Document1 paginăHitachi Solutions - ETIQA - Application Form (Signed)Bernard CasimiroÎncă nu există evaluări
- Neuroleptic Malignant Syndrome (NMS)Document21 paginiNeuroleptic Malignant Syndrome (NMS)Aditya ChhabraÎncă nu există evaluări
- RA For Installation & Dismantling of Loading Platform A69Document8 paginiRA For Installation & Dismantling of Loading Platform A69Sajid ShahÎncă nu există evaluări
- Community Health Nursing Approach: Mrs - Neethu Vincent Asst Professor KVM College of NursingDocument21 paginiCommunity Health Nursing Approach: Mrs - Neethu Vincent Asst Professor KVM College of NursingNeethu VincentÎncă nu există evaluări
- Civil Liberties and Civil Commitment: The Therapeutic State by Thomas SzaszDocument2 paginiCivil Liberties and Civil Commitment: The Therapeutic State by Thomas SzaszAbdelrahman Abdallah TI from London RIPÎncă nu există evaluări
- Disturbed Sleep pattern-NCPDocument2 paginiDisturbed Sleep pattern-NCPLADY CLAIRE DOBLEÎncă nu există evaluări
- PASSMED MRCP MCQs-DERMATOLOGY PDFDocument53 paginiPASSMED MRCP MCQs-DERMATOLOGY PDFFatima Ema100% (5)
- IGC3 Exam Template 2Document17 paginiIGC3 Exam Template 2mibshÎncă nu există evaluări
- Erythrocytosis PolycythemiaDocument2 paginiErythrocytosis PolycythemiaNeoMedica100% (2)