S-ar putea să vă placă și
- Nursing Diagnosis For AsthmaDocument6 paginiNursing Diagnosis For AsthmaTINAIDA33% (3)
- NCP - TBDocument2 paginiNCP - TBPahw BaluisÎncă nu există evaluări
- NCP TBDocument6 paginiNCP TBGrhace Aquino100% (3)
- NCP For FeverDocument2 paginiNCP For FeverDominises Jade Corpuz82% (17)
- Decreased Cardiac OutputDocument3 paginiDecreased Cardiac OutputRizalyn QuindipanÎncă nu există evaluări
- Hiv NCPDocument2 paginiHiv NCPHeindrich Cardenas0% (1)
- NCP EmphysemaDocument9 paginiNCP Emphysemahermesdave188% (8)
- NCP PneumoniaDocument3 paginiNCP Pneumoniakaiserdominick100% (2)
- Impaired Gas ExchangeDocument2 paginiImpaired Gas ExchangeAura Salve Ildefonso Allas100% (3)
- NCP AidsDocument16 paginiNCP AidstferdianingsihÎncă nu există evaluări
- 3 NCP AsthmaDocument6 pagini3 NCP AsthmajaninenicoleÎncă nu există evaluări
- NCP - Diarrhea - FeunrmfDocument7 paginiNCP - Diarrhea - FeunrmfJk SalvadorÎncă nu există evaluări
- NCP TyphoidDocument4 paginiNCP TyphoidFate ZephyrÎncă nu există evaluări
- Date/ Time Cues Nee D Nursing Diagnosis Patient Outcome Nursing Interventions Impleme N Tation EvaluationDocument3 paginiDate/ Time Cues Nee D Nursing Diagnosis Patient Outcome Nursing Interventions Impleme N Tation EvaluationJennifer Davis CondimanÎncă nu există evaluări
- Nursing Care Plan For AIDS HIVDocument3 paginiNursing Care Plan For AIDS HIVFARAH MAE MEDINA100% (2)
- NCP TuberculosisDocument3 paginiNCP TuberculosisAnonymous XvwKtnSrMR50% (2)
- NCP-Deficient Fluid VolumeDocument1 paginăNCP-Deficient Fluid Volumejanmichael8Încă nu există evaluări
- NCP Difficulty of Breathing R/T SecretionDocument3 paginiNCP Difficulty of Breathing R/T Secretionherscentasiascribd50% (8)
- NCP - CopdDocument3 paginiNCP - CopdhystericoÎncă nu există evaluări
- Ineffective Breathing PatternDocument2 paginiIneffective Breathing PatternJoy Arizala CarasiÎncă nu există evaluări
- Pneumonia-Ineffective Airway ClearanceDocument2 paginiPneumonia-Ineffective Airway ClearanceNursesLabs.com86% (7)
- 2NF - Grand Case Presentation Written OutputDocument99 pagini2NF - Grand Case Presentation Written OutputKyra Bianca R. FamacionÎncă nu există evaluări
- Copd NCPDocument16 paginiCopd NCPSuperMaye100% (1)
- Ineffective Airway Clearance Related To BronchospasmDocument2 paginiIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- Fixcom 4Document2 paginiFixcom 4Jenny Vi Codeniera100% (2)
- NURSING CARE PLAN For TB 2003Document6 paginiNURSING CARE PLAN For TB 2003Princess Andrea Bulatao100% (1)
- Gallstone NCPDocument2 paginiGallstone NCPKelly RiedingerÎncă nu există evaluări
- NCP For PCAPCDocument6 paginiNCP For PCAPCEnrique Lu100% (1)
- Defining Characteristics Nursing Diagnosis Scientifc Analysis Plan of Care Nursing Interventions RationaleDocument3 paginiDefining Characteristics Nursing Diagnosis Scientifc Analysis Plan of Care Nursing Interventions Rationalesbo100% (1)
- Ineffective Breathing PatternDocument8 paginiIneffective Breathing PatternJansen Arquilita Rivera100% (2)
- Nursing Care Plan For Pneumonia NCPDocument2 paginiNursing Care Plan For Pneumonia NCPRoger Jr PumarenÎncă nu există evaluări
- Pathophysiology PTBDocument1 paginăPathophysiology PTBNikki Galvez Braganza100% (2)
- Electrolyte Imbalance NCPDocument8 paginiElectrolyte Imbalance NCPManuel Jacob YradÎncă nu există evaluări
- NCP Cushing's SyndromeDocument2 paginiNCP Cushing's SyndromeChristine LebicoÎncă nu există evaluări
- NCP Pathophysiology Acute PyelonephritisDocument20 paginiNCP Pathophysiology Acute PyelonephritisChristine Karen Ang Suarez100% (2)
- SAMPLE NCP For Angina PectorisDocument3 paginiSAMPLE NCP For Angina Pectorisseanne_may100% (4)
- Novilyn C. Pataray BSN - Ii Cystic Fibrosis: St. Paul College of Ilocos SurDocument1 paginăNovilyn C. Pataray BSN - Ii Cystic Fibrosis: St. Paul College of Ilocos SurCharina AubreyÎncă nu există evaluări
- NCPDocument8 paginiNCPJoseph Anthony Benitez VerzosaÎncă nu există evaluări
- Nursing Care Plan:: Lopez, Maria Sofia B. 10/18/2020 3-BSN-B Prof. IsananDocument4 paginiNursing Care Plan:: Lopez, Maria Sofia B. 10/18/2020 3-BSN-B Prof. IsananSofia LopezÎncă nu există evaluări
- NCP CopdDocument6 paginiNCP Copdjoelette100% (1)
- NCP For UtiDocument3 paginiNCP For UtiAaron Sanchez100% (1)
- Case Study Part 2 Patient With Uti (Bag-O)Document48 paginiCase Study Part 2 Patient With Uti (Bag-O)Eaht Quirong0% (1)
- Nicu NCP (Neo - Pnia)Document3 paginiNicu NCP (Neo - Pnia)lorence_cachoÎncă nu există evaluări
- Hyperthermia Pneumonia Nursing Care PlanDocument1 paginăHyperthermia Pneumonia Nursing Care Planjustin_saneÎncă nu există evaluări
- NCP Ineffective Airway Clearance ChildDocument3 paginiNCP Ineffective Airway Clearance ChildMarion Delos SantosÎncă nu există evaluări
- Deficit)Document2 paginiDeficit)Lee DeeÎncă nu există evaluări
- Acc Phu Case NCP HyperthermiaDocument1 paginăAcc Phu Case NCP Hyperthermiamacy_bautistaÎncă nu există evaluări
- Care Plan ExampleDocument2 paginiCare Plan Exampleincess27100% (1)
- NCP UtiDocument2 paginiNCP UtiyasiraÎncă nu există evaluări
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument4 paginiAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- NCP Imbalanced NutritionDocument3 paginiNCP Imbalanced NutritionAav Canlas100% (1)
- NCPDocument4 paginiNCPAndrea BroccoliÎncă nu există evaluări
- Chronic Obstructive Bronchitis Is An Inflammation of The BronchiDocument9 paginiChronic Obstructive Bronchitis Is An Inflammation of The Bronchiinamaliit100% (1)
- CJ C J CJ CJ Cî CJ CJ C C ! "! Cî C Ë # C Ë # CJ$ C C 0 "% C C & C C C Ë Î C "' (C Ëj "ËjDocument105 paginiCJ C J CJ CJ Cî CJ CJ C C ! "! Cî C Ë # C Ë # CJ$ C C 0 "% C C & C C C Ë Î C "' (C Ëj "ËjShirin Forbes Aquino100% (2)
- NCP For Pleural EffusionDocument4 paginiNCP For Pleural EffusionLilian Linogao71% (7)
- Nursing Care of Patients With HIV-AIDSDocument37 paginiNursing Care of Patients With HIV-AIDSKiki SeptyantiÎncă nu există evaluări
- Chronic Obstructive Pulmonary Disease (COPD)Document1 paginăChronic Obstructive Pulmonary Disease (COPD)Bheru LalÎncă nu există evaluări
- 1 Ineffective Breathing PatternDocument7 pagini1 Ineffective Breathing PatternKrisJane Ratilla Abiva100% (2)
- NCPDocument9 paginiNCPEjie Boy Isaga67% (3)
- Ncp's FOR PLEURAL EFFUSIONDocument4 paginiNcp's FOR PLEURAL EFFUSIONHania Polangi100% (1)
- Daftar Harga ObatDocument2 paginiDaftar Harga ObatHadi SetiawanÎncă nu există evaluări
- JAM2Document80 paginiJAM2Nicoleta Florentina GhencianÎncă nu există evaluări
- Requirement IN Psychiatric Nursing: Gencris M. Giray Bsn-3ADocument5 paginiRequirement IN Psychiatric Nursing: Gencris M. Giray Bsn-3AGencris Medrano Giray RN100% (2)
- Vasculitis Syndrome (VS) : Dr. Julius Roma, SP ADocument45 paginiVasculitis Syndrome (VS) : Dr. Julius Roma, SP ADavid ChristianÎncă nu există evaluări
- UntitledDocument213 paginiUntitledNaynesh Patel100% (2)
- Tema 4 Qwiz 3 F.S.Document3 paginiTema 4 Qwiz 3 F.S.Top MusicÎncă nu există evaluări
- Aerobic Exercise: Marching in PlaceDocument4 paginiAerobic Exercise: Marching in Placenemica tamayaoÎncă nu există evaluări
- HypoglicemiaDocument4 paginiHypoglicemiayeniÎncă nu există evaluări
- ParenteralDocument10 paginiParenteralDennis SantosÎncă nu există evaluări
- Tai Chi For Health PurposesDocument7 paginiTai Chi For Health PurposesClaire18Încă nu există evaluări
- Self-Hypnosis For Personal Creativity PDFDocument91 paginiSelf-Hypnosis For Personal Creativity PDFKalil Morais Martins100% (6)
- Assembling and Disassembling Oxygen RegulatorDocument23 paginiAssembling and Disassembling Oxygen RegulatorBryan DorosanÎncă nu există evaluări
- Implicit Memory and MetacognitionDocument22 paginiImplicit Memory and MetacognitionMonica SanduleanuÎncă nu există evaluări
- Neurogenesis: The Amygdala and The HippocampusDocument3 paginiNeurogenesis: The Amygdala and The HippocampusAnonymous j3gtTw100% (1)
- Kisi-Kisi Tes Masuk Ppds Bedah Umum Fkui April 2011Document18 paginiKisi-Kisi Tes Masuk Ppds Bedah Umum Fkui April 2011David SantosoÎncă nu există evaluări
- Preventive DentistryDocument3 paginiPreventive DentistryMoataz Mohamed BarakatÎncă nu există evaluări
- Parallel Process in Psychotherapy Supervision PDFDocument5 paginiParallel Process in Psychotherapy Supervision PDFМайя МладеноваÎncă nu există evaluări
- Jpracticals in Pharmaceutical Technology 2011Document260 paginiJpracticals in Pharmaceutical Technology 2011KatalinÎncă nu există evaluări
- Admission:Discharge Criteria in Speech-Language Pathology - ASHADocument16 paginiAdmission:Discharge Criteria in Speech-Language Pathology - ASHANádia MarquesÎncă nu există evaluări
- Therapeutics PlanningDocument13 paginiTherapeutics PlanningCésar Augusto Sánchez SolisÎncă nu există evaluări
- Course Syllabus - Abnormal PsychologyDocument2 paginiCourse Syllabus - Abnormal Psychologyapi-3855346Încă nu există evaluări
- Word HNPDocument14 paginiWord HNPALan ButukÎncă nu există evaluări
- Case PresentationDocument34 paginiCase PresentationgpstÎncă nu există evaluări
- Activities Specific Balance Confidence ScaleDocument2 paginiActivities Specific Balance Confidence Scalerk_s7Încă nu există evaluări
- SW 7070 Group Presentation 1Document28 paginiSW 7070 Group Presentation 1api-368489332Încă nu există evaluări
- Mercy Hospital - Crystal Lake ReviewDocument33 paginiMercy Hospital - Crystal Lake ReviewNorthwest HeraldÎncă nu există evaluări
- Purifying LimeDocument19 paginiPurifying LimeNazihCosmeticsÎncă nu există evaluări
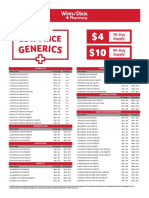
- Generic DrugsDocument2 paginiGeneric DrugsWendy StarkandÎncă nu există evaluări
- Sequential Compression DeviceDocument2 paginiSequential Compression Deviceal-obinay shereen0% (1)
- Progressive Primary Pulmonary TB in A 15-Month Old ChildDocument1 paginăProgressive Primary Pulmonary TB in A 15-Month Old ChildRenierose AgujetasÎncă nu există evaluări