S-ar putea să vă placă și
- ESI Certificate for Medical LeaveDocument1 paginăESI Certificate for Medical LeaveUmesh C0% (1)
- Sickness Self-Certification FormDocument1 paginăSickness Self-Certification FormDaniela GrosuÎncă nu există evaluări
- Employees' State Insurance Corporation: Strike Out If Not ApplicableDocument1 paginăEmployees' State Insurance Corporation: Strike Out If Not Applicablenasir ahmedÎncă nu există evaluări
- Employees' State Insurance Corporation: Strike Out If Not ApplicableDocument1 paginăEmployees' State Insurance Corporation: Strike Out If Not Applicablenasir ahmedÎncă nu există evaluări
- Aia Form 1 PDFDocument3 paginiAia Form 1 PDFVicky PascuaÎncă nu există evaluări
- Application for Disability Retirement FormDocument4 paginiApplication for Disability Retirement FormGianJyrellAlbertoCorletÎncă nu există evaluări
- Esic Claim Sickness Form9Document1 paginăEsic Claim Sickness Form9trupti_naik08725Încă nu există evaluări
- Maternity Leave Application Form Performa PDFDocument4 paginiMaternity Leave Application Form Performa PDFAnonymous epg6ult78% (9)
- Form 14Document1 paginăForm 14hdpanchal86100% (1)
- Borang Manfaat Hospital TerkiniDocument5 paginiBorang Manfaat Hospital Terkiniabdul malik abdul wahidÎncă nu există evaluări
- Medical Claim Form (Family TakafulDocument4 paginiMedical Claim Form (Family TakafulFathi TahirÎncă nu există evaluări
- Form Claim Section A - Med ExDocument4 paginiForm Claim Section A - Med Exerwin hpÎncă nu există evaluări
- FORM – 2 FINAL PAYMENT APPLICATIONDocument7 paginiFORM – 2 FINAL PAYMENT APPLICATIONSelva KumarÎncă nu există evaluări
- Agrahara Claim Form (English)Document14 paginiAgrahara Claim Form (English)hema160% (1)
- FORM 6 (A) Form of Application For Final Payment of Balances in The General Provident Fund AccountDocument4 paginiFORM 6 (A) Form of Application For Final Payment of Balances in The General Provident Fund AccountHarish PlÎncă nu există evaluări
- Statutory Declaration FormDocument3 paginiStatutory Declaration Formmackcaslangan08Încă nu există evaluări
- Sicknessandfitnesscertificates PDFDocument6 paginiSicknessandfitnesscertificates PDFniraj_sdÎncă nu există evaluări
- Agrahara Claim Form (English)Document16 paginiAgrahara Claim Form (English)Gayan Indunil Jayasundara50% (2)
- General Consent FormDocument2 paginiGeneral Consent FormBernewsAdminÎncă nu există evaluări
- Indiafirst Life CSC "Insurance Khata" Plan: Instructions For Filling The FormDocument2 paginiIndiafirst Life CSC "Insurance Khata" Plan: Instructions For Filling The FormSHAHID MALIKÎncă nu există evaluări
- UIIC Claim FormDocument4 paginiUIIC Claim FormDevang TailorÎncă nu există evaluări
- 5.letter of Good StandingDocument6 pagini5.letter of Good Standingkayzinhtaik100% (3)
- Passport No Objection CertificateDocument8 paginiPassport No Objection CertificateRenuga DeviÎncă nu există evaluări
- Death Claimant StatementDocument4 paginiDeath Claimant Statementcet.ranchi7024Încă nu există evaluări
- RegistrationDocument4 paginiRegistrationruksfarhanÎncă nu există evaluări
- Health Claim Intimation FormDocument3 paginiHealth Claim Intimation FormKiranmayi UppalaÎncă nu există evaluări
- GPF Final PaymentDocument2 paginiGPF Final PaymentRanga Nayak PaltyaÎncă nu există evaluări
- Reimbursement Claim Form of National Insurance CompnayDocument4 paginiReimbursement Claim Form of National Insurance CompnayVidya Sagar TamminaÎncă nu există evaluări
- Form-19 Claim for Maternity BenefitDocument2 paginiForm-19 Claim for Maternity BenefitMujibur RehmanÎncă nu există evaluări
- Resident Physician Medicine JobDocument7 paginiResident Physician Medicine JobEngr Md. Mamun RassalÎncă nu există evaluări
- The Employees State Insurance Act, 1948Document24 paginiThe Employees State Insurance Act, 1948Pawan KumarÎncă nu există evaluări
- Borang ADocument13 paginiBorang AZahirah Rashid KhanÎncă nu există evaluări
- Claim 20formDocument1 paginăClaim 20formkamaleshvmÎncă nu există evaluări
- ESIC Certificate of Entitlement and Medical Treatment FormDocument2 paginiESIC Certificate of Entitlement and Medical Treatment FormIndustrial Security Agency90% (10)
- Form 10Document3 paginiForm 10hdpanchal86Încă nu există evaluări
- PC-(Levying of Fees and Registration of Pharmacists) Regulations 2017-annotated GrequinDocument9 paginiPC-(Levying of Fees and Registration of Pharmacists) Regulations 2017-annotated Grequingrsrequin48Încă nu există evaluări
- Contract of Employment SbaDocument2 paginiContract of Employment SbaMellia EmmanuelÎncă nu există evaluări
- Renew Your Physiotherapy LicenseDocument3 paginiRenew Your Physiotherapy LicenseShrikant SantÎncă nu există evaluări
- PPF Forms for Opening, Nomination and Loan ApplicationDocument9 paginiPPF Forms for Opening, Nomination and Loan ApplicationVivek Godgift JÎncă nu există evaluări
- Contract Employment Junior Day CareDocument8 paginiContract Employment Junior Day CareCalvinhoÎncă nu există evaluări
- TAMILNADU MEDICAL COUNCIL ADVISORY ON MEDICAL CERTIFICATESDocument4 paginiTAMILNADU MEDICAL COUNCIL ADVISORY ON MEDICAL CERTIFICATESSharavana KumarÎncă nu există evaluări
- ClaimApplicalionFormGS EDocument5 paginiClaimApplicalionFormGS ERavi JanakaÎncă nu există evaluări
- Industrial Commission of Arizona: Workers' Compensation Information For The Injured WorkerDocument12 paginiIndustrial Commission of Arizona: Workers' Compensation Information For The Injured WorkerdejewsonÎncă nu există evaluări
- Joining Induction FormDocument24 paginiJoining Induction FormAnaruzzaman SheikhÎncă nu există evaluări
- Form LeavesDocument1 paginăForm LeavesEFFAÎncă nu există evaluări
- Form 13Document1 paginăForm 13hdpanchal86Încă nu există evaluări
- CVC: PNB Awarded For Timely Completion of Disciplinary Proceedings ..Document5 paginiCVC: PNB Awarded For Timely Completion of Disciplinary Proceedings ..Shri Gopal SoniÎncă nu există evaluări
- Holiday Request 27-Apr-28-Apr2023Document1 paginăHoliday Request 27-Apr-28-Apr2023Melissa MirandaÎncă nu există evaluări
- Self Declaration For Issue of COPDocument2 paginiSelf Declaration For Issue of COPNitin CSÎncă nu există evaluări
- Claimant Statement Form Death Claim 2Document3 paginiClaimant Statement Form Death Claim 2Anitha AnuÎncă nu există evaluări
- Contract of Employment For Factory Workers From Sri Lanka (Private Recruitment)Document4 paginiContract of Employment For Factory Workers From Sri Lanka (Private Recruitment)vantaradubaiÎncă nu există evaluări
- How To Avail Benefits Under ESIC ActDocument3 paginiHow To Avail Benefits Under ESIC ActVishnu MuraleedharanÎncă nu există evaluări
- Voluntary SssDocument5 paginiVoluntary SssRaissa Anjela Carman-JardenicoÎncă nu există evaluări
- Medical-leave-proforma-20200612132007_2_2Document4 paginiMedical-leave-proforma-20200612132007_2_2besttubergamersÎncă nu există evaluări
- Shlok Tripathi Aphthous ulcersDocument4 paginiShlok Tripathi Aphthous ulcersbesttubergamersÎncă nu există evaluări
- FORM-1-A: Present Postal Address . .., Postal Address After RetirementDocument3 paginiFORM-1-A: Present Postal Address . .., Postal Address After RetirementAnonymous 7CITEMBPÎncă nu există evaluări
- Andhra Pradesh Medical Council: See Section-15C of A.P Medical Practitioners Registration (Amendment) Act, 2013Document3 paginiAndhra Pradesh Medical Council: See Section-15C of A.P Medical Practitioners Registration (Amendment) Act, 2013kirank_11Încă nu există evaluări
- Employee Dismissal: Practical Solutions for EmployersDe la EverandEmployee Dismissal: Practical Solutions for EmployersÎncă nu există evaluări
- SERIES 63 EXAM STUDY GUIDE 2022 + TEST BANKDe la EverandSERIES 63 EXAM STUDY GUIDE 2022 + TEST BANKÎncă nu există evaluări
- All Form - Minimum Wages ActDocument12 paginiAll Form - Minimum Wages Acthdpanchal86Încă nu există evaluări
- ER-1 Quarterly ReturnDocument2 paginiER-1 Quarterly Returnhdpanchal86Încă nu există evaluări
- Notice of Minimum WagesDocument1 paginăNotice of Minimum Wageshdpanchal86Încă nu există evaluări
- Form III - Annual ReturnDocument2 paginiForm III - Annual Returnhdpanchal86Încă nu există evaluări
- Format PF 5.10.12Document6 paginiFormat PF 5.10.12hdpanchal86Încă nu există evaluări
- Form - E - Work TimingDocument2 paginiForm - E - Work Timinghdpanchal86Încă nu există evaluări
- Form - I - Over TimeDocument2 paginiForm - I - Over Timehdpanchal86Încă nu există evaluări
- All Forms - Mines Vocational Training Rules 1966Document39 paginiAll Forms - Mines Vocational Training Rules 1966hdpanchal8675% (4)
- Form - L - Information Regarding Leave With WagesDocument2 paginiForm - L - Information Regarding Leave With Wageshdpanchal86Încă nu există evaluări
- Form - B - Register of EmployeesDocument1 paginăForm - B - Register of Employeeshdpanchal86Încă nu există evaluări
- Form - G - Register of Leave Account During The Calendar Year 2012Document16 paginiForm - G - Register of Leave Account During The Calendar Year 2012hdpanchal86Încă nu există evaluări
- FORM IV - Register of Advances Made To Employed PersonsDocument1 paginăFORM IV - Register of Advances Made To Employed Personshdpanchal86Încă nu există evaluări
- Form - H - Leave With WagesDocument1 paginăForm - H - Leave With Wageshdpanchal86100% (3)
- Form - F - Register of Compensatory Days of RestDocument4 paginiForm - F - Register of Compensatory Days of Resthdpanchal860% (1)
- Form - A - Notice of Commencement & End of WorkDocument2 paginiForm - A - Notice of Commencement & End of Workhdpanchal86Încă nu există evaluări
- Er IiDocument3 paginiEr Iihdpanchal86Încă nu există evaluări
- Form - N - Prosecution During The Year EndingDocument1 paginăForm - N - Prosecution During The Year Endinghdpanchal86Încă nu există evaluări
- Form Er 1Document3 paginiForm Er 1hdpanchal8625% (4)
- Form L - SampleDocument2 paginiForm L - Samplehdpanchal86Încă nu există evaluări
- Form M Under Maternity Benefit ActDocument1 paginăForm M Under Maternity Benefit Acthdpanchal860% (1)
- Form D, Annual Return Under Payement of Bonus ActDocument2 paginiForm D, Annual Return Under Payement of Bonus ActSatyam mishraÎncă nu există evaluări
- Form IV - Annual ReturnDocument2 paginiForm IV - Annual Returnhdpanchal86Încă nu există evaluări
- Form A, B & C - Bonus ActDocument8 paginiForm A, B & C - Bonus Acthdpanchal86Încă nu există evaluări
- Form L Under Maternity Benefit ActDocument1 paginăForm L Under Maternity Benefit Acthdpanchal86100% (1)
- The Maternity Benefit Act Forms & RegistersDocument1 paginăThe Maternity Benefit Act Forms & Registershdpanchal86Încă nu există evaluări
- Form K Under Maternity Benefit ActDocument1 paginăForm K Under Maternity Benefit Acthdpanchal8660% (5)
- FORM - H - Modification of NominationDocument2 paginiFORM - H - Modification of Nominationhdpanchal86Încă nu există evaluări
- FORM F NominationDocument2 paginiFORM F Nominationhdpanchal86Încă nu există evaluări
- FORM - G - Fresh NominationDocument2 paginiFORM - G - Fresh Nominationhdpanchal86Încă nu există evaluări
- FORM - E - Notice of Withdrawal of Notice Excluding Husband From FamilyDocument1 paginăFORM - E - Notice of Withdrawal of Notice Excluding Husband From Familyhdpanchal86Încă nu există evaluări
- 9IMJan 4477 1Document9 pagini9IMJan 4477 1Upasana PadhiÎncă nu există evaluări
- 5.PassLeader 210-260 Exam Dumps (121-150)Document9 pagini5.PassLeader 210-260 Exam Dumps (121-150)Shaleh SenÎncă nu există evaluări
- Tata Group's Global Expansion and Business StrategiesDocument23 paginiTata Group's Global Expansion and Business Strategiesvgl tamizhÎncă nu există evaluări
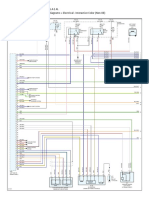
- 1990-1994 Electrical Wiring - DiagramsDocument13 pagini1990-1994 Electrical Wiring - Diagramsal exÎncă nu există evaluări
- ITSCM Mindmap v4Document1 paginăITSCM Mindmap v4Paul James BirchallÎncă nu există evaluări
- MCDO of Diesel Shed, AndalDocument12 paginiMCDO of Diesel Shed, AndalUpendra ChoudharyÎncă nu există evaluări
- Flare Finance Ecosystem MapDocument1 paginăFlare Finance Ecosystem MapEssence of ChaÎncă nu există evaluări
- Course Syllabus: Aurora Pioneers Memorial CollegeDocument9 paginiCourse Syllabus: Aurora Pioneers Memorial CollegeLorisa CenizaÎncă nu există evaluări
- 21st Century LiteraciesDocument27 pagini21st Century LiteraciesYuki SeishiroÎncă nu există evaluări
- "60 Tips On Object Oriented Programming" BrochureDocument1 pagină"60 Tips On Object Oriented Programming" BrochuresgganeshÎncă nu există evaluări
- Area Access Manager (Browser-Based Client) User GuideDocument22 paginiArea Access Manager (Browser-Based Client) User GuideKatherineÎncă nu există evaluări
- Guidelines On Accreditation of CSOs (LSB Representation) - DILG MC 2019-72Document18 paginiGuidelines On Accreditation of CSOs (LSB Representation) - DILG MC 2019-72Cedric Dequito100% (1)
- Elaspeed Cold Shrink Splices 2010Document3 paginiElaspeed Cold Shrink Splices 2010moisesramosÎncă nu există evaluări
- OBHR Case StudyDocument8 paginiOBHR Case StudyYvonne TanÎncă nu există evaluări
- The Human Resource Department of GIK InstituteDocument1 paginăThe Human Resource Department of GIK InstitutexandercageÎncă nu există evaluări
- 2CG ELTT2 KS TitanMagazine Anazelle-Shan PromoDocument12 pagini2CG ELTT2 KS TitanMagazine Anazelle-Shan PromoJohn SmithÎncă nu există evaluări
- Engine Controls (Powertrain Management) - ALLDATA RepairDocument4 paginiEngine Controls (Powertrain Management) - ALLDATA Repairmemo velascoÎncă nu există evaluări
- 13-07-01 Declaration in Support of Skyhook Motion To CompelDocument217 pagini13-07-01 Declaration in Support of Skyhook Motion To CompelFlorian MuellerÎncă nu există evaluări
- Magnetism 02Document10 paginiMagnetism 02Niharika DeÎncă nu există evaluări
- Leg Wri FInal ExamDocument15 paginiLeg Wri FInal ExamGillian CalpitoÎncă nu există evaluări
- Janapriya Journal of Interdisciplinary Studies - Vol - 6Document186 paginiJanapriya Journal of Interdisciplinary Studies - Vol - 6abiskarÎncă nu există evaluări
- 1 Estafa - Arriola Vs PeopleDocument11 pagini1 Estafa - Arriola Vs PeopleAtty Richard TenorioÎncă nu există evaluări
- CAP Regulation 20-1 - 05/29/2000Document47 paginiCAP Regulation 20-1 - 05/29/2000CAP History LibraryÎncă nu există evaluări
- Overall Dimensions and Mounting: Solar Water Pump Controller Mu - G3 Solar Mu - G5 Solar Mu - G7.5 Solar Mu - G10 SolarDocument2 paginiOverall Dimensions and Mounting: Solar Water Pump Controller Mu - G3 Solar Mu - G5 Solar Mu - G7.5 Solar Mu - G10 SolarVishak ThebossÎncă nu există evaluări
- Mba Assignment SampleDocument5 paginiMba Assignment Sampleabdallah abdÎncă nu există evaluări
- PS300-TM-330 Owners Manual PDFDocument55 paginiPS300-TM-330 Owners Manual PDFLester LouisÎncă nu există evaluări
- Gary Mole and Glacial Energy FraudDocument18 paginiGary Mole and Glacial Energy Fraudskyy22990% (1)
- Shoib CV Scaffold EngineerDocument3 paginiShoib CV Scaffold EngineerMohd Shoib100% (1)
- EFM2e, CH 03, SlidesDocument36 paginiEFM2e, CH 03, SlidesEricLiangtoÎncă nu există evaluări
- Diagnostic Information For Database Replay IssuesDocument10 paginiDiagnostic Information For Database Replay IssuesjjuniorlopesÎncă nu există evaluări