S-ar putea să vă placă și
- IV Insulin Infusion Protocol TexasDocument2 paginiIV Insulin Infusion Protocol TexasJohb CaballeroÎncă nu există evaluări
- Role of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy LestariDocument32 paginiRole of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy Lestaridesy lestariÎncă nu există evaluări
- PEWS Training IndonesiaDocument36 paginiPEWS Training IndonesiaBbenq Prasetyo100% (1)
- Algoritma HiperkalemiaDocument1 paginăAlgoritma HiperkalemiaanrihmÎncă nu există evaluări
- Hipertensi Emergensi (Herbesser)Document41 paginiHipertensi Emergensi (Herbesser)riski novika100% (1)
- Gir (Glucose Infussion Rate)Document9 paginiGir (Glucose Infussion Rate)arawindahaniastriÎncă nu există evaluări
- Aida JNNS 25 Sept 2021-Anemia CKDDocument36 paginiAida JNNS 25 Sept 2021-Anemia CKDLaurensia Erlina NataliaÎncă nu există evaluări
- Sarcopenia and Osteoporosis-Terkunci PDFDocument33 paginiSarcopenia and Osteoporosis-Terkunci PDFNur AisyahÎncă nu există evaluări
- Otsuka CairanDocument60 paginiOtsuka Cairan_LipRaa_Încă nu există evaluări
- Congenital Adrenal HyperplasiaDocument14 paginiCongenital Adrenal HyperplasiabangkitayuÎncă nu există evaluări
- Thrombolisis Dan Trombektomi Pada Stroke AkutDocument48 paginiThrombolisis Dan Trombektomi Pada Stroke AkutanisÎncă nu există evaluări
- Perioperative Management OF Brain Trauma: Tatang Bisri Konsultan Neuroanestesi IDSAIDocument52 paginiPerioperative Management OF Brain Trauma: Tatang Bisri Konsultan Neuroanestesi IDSAIKimbek BuangkeÎncă nu există evaluări
- Tatalaksana Krisis HipertensiDocument38 paginiTatalaksana Krisis HipertensiDr Edi HidayatÎncă nu există evaluări
- Dr. Dr. Tri Maharani, M.si., Sp. em - Snake Bite Medical Management CrebonDocument33 paginiDr. Dr. Tri Maharani, M.si., Sp. em - Snake Bite Medical Management Crebonrio100% (1)
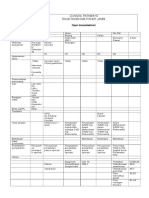
- Clinical Pathway Open CholecystektomiDocument2 paginiClinical Pathway Open CholecystektomiAnton TrihartantoÎncă nu există evaluări
- LEADING ARTICLE Inlacin Therapy in Patients With Type-2 Diabetes MellitusDocument10 paginiLEADING ARTICLE Inlacin Therapy in Patients With Type-2 Diabetes MellitusBabanx Reigncary100% (1)
- Steps EchoDocument2 paginiSteps EchoBagus Andi PramonoÎncă nu există evaluări
- Enok Algoritma Trauma Tumpul AbdomenDocument1 paginăEnok Algoritma Trauma Tumpul AbdomenhafidaoktaviaÎncă nu există evaluări
- Ozid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Document15 paginiOzid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Galih Aryo UtomoÎncă nu există evaluări
- Krisis Hipertensi IMELSDocument43 paginiKrisis Hipertensi IMELSrinadi_aÎncă nu există evaluări
- Anemia & HemobionDocument56 paginiAnemia & HemobionMar'atus SholikahÎncă nu există evaluări
- Anemia Pada CKD - 2015Document61 paginiAnemia Pada CKD - 2015Anonymous wVgEAr6Încă nu există evaluări
- (CKD-MBD) : Chronic Kidney Disease - Mineral and Bone DisorderDocument41 pagini(CKD-MBD) : Chronic Kidney Disease - Mineral and Bone DisorderronyheryadiÎncă nu există evaluări
- BGA Acid Base Stepwise PradikDocument43 paginiBGA Acid Base Stepwise PradikZulfadly NuralimÎncă nu există evaluări
- Farmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDocument45 paginiFarmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDark BlueÎncă nu există evaluări
- Diagnosis & Tata Laksana Cad / CcsDocument40 paginiDiagnosis & Tata Laksana Cad / CcsIno HajrinÎncă nu există evaluări
- Anemia in Chronic Kidney DiseaseDocument38 paginiAnemia in Chronic Kidney DiseaseHemodialisa LindimaraÎncă nu există evaluări
- Materi PP Aminofluid (Interna)Document16 paginiMateri PP Aminofluid (Interna)ajieÎncă nu există evaluări
- Algorithm For Management of Acute Pulmonary Oedema PDFDocument1 paginăAlgorithm For Management of Acute Pulmonary Oedema PDFDewi Rabiatul AkhzamiÎncă nu există evaluări
- Hepatorenal SyndromeDocument6 paginiHepatorenal SyndromeEveline YÎncă nu există evaluări
- Obat Obat HipertensiDocument74 paginiObat Obat HipertensiIlham Habib DjarkoniÎncă nu există evaluări
- Nutrition Support in Critically Ill PatientDocument19 paginiNutrition Support in Critically Ill PatienttantoÎncă nu există evaluări
- Gagal Ginjal Akut Dan Kronik: Divisi Ginjal & Hipertensi SMF/Lab - Ilmu Penyakit Dalam FK - UNS / RSUD DR - MoewardiDocument29 paginiGagal Ginjal Akut Dan Kronik: Divisi Ginjal & Hipertensi SMF/Lab - Ilmu Penyakit Dalam FK - UNS / RSUD DR - MoewardiHabiby Habibaty QolbiÎncă nu există evaluări
- Scoring RtPADocument2 paginiScoring RtPAeko aÎncă nu există evaluări
- Materi DR Rita Zahara NewDocument31 paginiMateri DR Rita Zahara NewIrfanÎncă nu există evaluări
- Encephalopaty UremicDocument6 paginiEncephalopaty UremicMasriyaniÎncă nu există evaluări
- (Mantap) Slide Materi Bedah-2 Batch 3 2018 PDFDocument200 pagini(Mantap) Slide Materi Bedah-2 Batch 3 2018 PDFRonald Shields100% (1)
- Airway Management (Covid 2021) - Yudi ElyasDocument63 paginiAirway Management (Covid 2021) - Yudi ElyasElsa Elsa LusariaÎncă nu există evaluări
- Eimed 2Document6 paginiEimed 2Herik Hamzah0% (4)
- Tarif Urologi Rs Tipe C Regional 1 2017Document10 paginiTarif Urologi Rs Tipe C Regional 1 2017NandarÎncă nu există evaluări
- Extubation Criteria & Delayed EmergenceDocument3 paginiExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwÎncă nu există evaluări
- Soal NeuroanatomiDocument92 paginiSoal NeuroanatomiGregorius Thomas PrasetiyoÎncă nu există evaluări
- Makalah Bhom 2018 PDFDocument354 paginiMakalah Bhom 2018 PDFAndrian KHoerul Anwar SiiGogon100% (2)
- Geriatric Syndromes: Dr. Sri Sunarti, SPPD K-Ger Divisi Geriatri Dan Gerontology Smf/Lab. Ipd Fkub/Rssa MalangDocument70 paginiGeriatric Syndromes: Dr. Sri Sunarti, SPPD K-Ger Divisi Geriatri Dan Gerontology Smf/Lab. Ipd Fkub/Rssa MalangrizqinapermatasariÎncă nu există evaluări
- Final 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteDocument67 paginiFinal 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteWirjapratama PutraÎncă nu există evaluări
- Dieckmann Et Al The PAT 1 PDFDocument4 paginiDieckmann Et Al The PAT 1 PDFLydia ElimÎncă nu există evaluări
- Vascular Acces in Hemodyalisi - DR DjoniDocument50 paginiVascular Acces in Hemodyalisi - DR DjoniMohamad ZulfikarÎncă nu există evaluări
- Different Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled TrialDocument8 paginiDifferent Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled Trialratnayanti udinÎncă nu există evaluări
- 2018 Farmakoterapi Obat-Obatan Emergency v2Document90 pagini2018 Farmakoterapi Obat-Obatan Emergency v2saifudinÎncă nu există evaluări
- RozerplastyDocument4 paginiRozerplastyLutfi Aulia RahmanÎncă nu există evaluări
- Lapsus Dr. DodyDocument36 paginiLapsus Dr. DodyPriscilla Christina NatanÎncă nu există evaluări
- Konsensus HipertiroidDocument6 paginiKonsensus HipertiroidDiethaKusumaningrumÎncă nu există evaluări
- Terapi Cairan Pada Pasien Shock HemooragikDocument41 paginiTerapi Cairan Pada Pasien Shock HemooragikNur Syifa FadhilahÎncă nu există evaluări
- CHYLOTHORAXDocument21 paginiCHYLOTHORAXZeerah Nor HazirahÎncă nu există evaluări
- Antibiotik Rasional Pada Demam TifoidDocument35 paginiAntibiotik Rasional Pada Demam TifoidSelvi SulistianingsihÎncă nu există evaluări
- Diabetes and NephrologyDocument36 paginiDiabetes and NephrologydrpbendreÎncă nu există evaluări
- Dr. Hikmat - Inisiasi Insulin CirebonDocument44 paginiDr. Hikmat - Inisiasi Insulin CirebonLukman SugiartoÎncă nu există evaluări
- Protocol For Intensive Intravenous Insulin Infusion For ICUDocument2 paginiProtocol For Intensive Intravenous Insulin Infusion For ICUburlacuraduuÎncă nu există evaluări
- Insulin in DMDocument46 paginiInsulin in DMask1400Încă nu există evaluări
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDe la EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesEvaluare: 4 din 5 stele4/5 (2)