S-ar putea să vă placă și
- Corporate Classic PDFDocument4 paginiCorporate Classic PDFironhide404Încă nu există evaluări
- TEMI880&850 Manual (Eng)Document122 paginiTEMI880&850 Manual (Eng)Mihir PrajapatiÎncă nu există evaluări
- Metlife - Dental Ppo 12 15Document3 paginiMetlife - Dental Ppo 12 15api-252555369Încă nu există evaluări
- Oxf Fre Access Ppo1b Ny f1Document1 paginăOxf Fre Access Ppo1b Ny f1Function0Încă nu există evaluări
- Questionnaire Exercise: Deals Desk Analyst Please Answer Below Questions and Email Your Responses Before First Technical Round of InterviewDocument2 paginiQuestionnaire Exercise: Deals Desk Analyst Please Answer Below Questions and Email Your Responses Before First Technical Round of InterviewAbhinav SahaniÎncă nu există evaluări
- Cognizant Company FAQDocument4 paginiCognizant Company FAQManojChowdary100% (1)
- 2021 - Life, Dental, Vision PacketDocument12 pagini2021 - Life, Dental, Vision PacketEberÎncă nu există evaluări
- 2015-16 Delta PPO Plan HighlightsDocument2 pagini2015-16 Delta PPO Plan HighlightsamberarunÎncă nu există evaluări
- APRIL 1, 2011: Preferred Blue PPO Plan Blue Care Elect PPODocument19 paginiAPRIL 1, 2011: Preferred Blue PPO Plan Blue Care Elect PPOIan S. SandovalÎncă nu există evaluări
- Our Dental Plan For Individuals and FamiliesDocument4 paginiOur Dental Plan For Individuals and Familiesapi-41207808Încă nu există evaluări
- New Hire Benefits Summary: Medical Plan OptionsDocument3 paginiNew Hire Benefits Summary: Medical Plan OptionsRavi Prakash MayreddyÎncă nu există evaluări
- Actives Association June12Document9 paginiActives Association June12Latisha WalkerÎncă nu există evaluări
- Ameritas Dental BrochureDocument4 paginiAmeritas Dental BrochureSocialmobile TrafficÎncă nu există evaluări
- Bupa GoldExtras NSW ACT 0415Document3 paginiBupa GoldExtras NSW ACT 0415Laura Leander WildeÎncă nu există evaluări
- 2011 BCBS PlansGlance PDFDocument2 pagini2011 BCBS PlansGlance PDFsakethram_gÎncă nu există evaluări
- HCF - Top PlusDocument14 paginiHCF - Top PluscraivaimÎncă nu există evaluări
- Individual Dental Comparison 93Document1 paginăIndividual Dental Comparison 93Anonymous rzioELmbrgÎncă nu există evaluări
- 2011-12 Benefits BrochureDocument4 pagini2011-12 Benefits BrochureKevin MarshallÎncă nu există evaluări
- 2024 Dental SummaryDocument5 pagini2024 Dental SummarySaravanan MuniandiÎncă nu există evaluări
- Humana Dental BrochureDocument4 paginiHumana Dental BrochureJeffrey PowellÎncă nu există evaluări
- IRIDA ANGJELI - DandHDistributing - Fall2011Document27 paginiIRIDA ANGJELI - DandHDistributing - Fall2011studentATtempleÎncă nu există evaluări
- Premier 2000 NWDocument2 paginiPremier 2000 NWacolyteÎncă nu există evaluări
- Spirit Dental PowerpointDocument21 paginiSpirit Dental PowerpointJohn BerkowitzÎncă nu există evaluări
- Ternian HCIS InteractiveDocument10 paginiTernian HCIS InteractivetrninsgrpÎncă nu există evaluări
- Employee Benefits-Wellness Guide 2023-24Document30 paginiEmployee Benefits-Wellness Guide 2023-24shanzeh2609Încă nu există evaluări
- GMHBA FactSheet G75 PDFDocument5 paginiGMHBA FactSheet G75 PDFLaura Leander WildeÎncă nu există evaluări
- Benefit Plan: Manulife Benefits BasicsDocument1 paginăBenefit Plan: Manulife Benefits BasicsMuneeb ArshadÎncă nu există evaluări
- Delta Dental Plan Compare Highlight SheetDocument2 paginiDelta Dental Plan Compare Highlight SheetTiffany BarnesÎncă nu există evaluări
- MC Card PP FinalDocument39 paginiMC Card PP FinalPuneeth kumar HSÎncă nu există evaluări
- Blue-Cross-Premier-Platinum-Extra-Dental-Vision CareerDocument8 paginiBlue-Cross-Premier-Platinum-Extra-Dental-Vision Careerapi-248930594Încă nu există evaluări
- 2022 1027 Ahs SD 1058-1 BroDocument8 pagini2022 1027 Ahs SD 1058-1 BroFernanda VargasÎncă nu există evaluări
- Insurance Benefit SummaryDocument4 paginiInsurance Benefit SummaryRose Mary Read BallÎncă nu există evaluări
- Bcbs HDHPPremierDocument2 paginiBcbs HDHPPremierTerry BybeeÎncă nu există evaluări
- So Cal Kaiser GuideDocument13 paginiSo Cal Kaiser GuideWai DaiÎncă nu există evaluări
- Your Customized Benefits Plan at HCL America IncDocument2 paginiYour Customized Benefits Plan at HCL America IncShiv RanjanÎncă nu există evaluări
- Carington Superior 1013 EditableDocument1 paginăCarington Superior 1013 Editableapi-288656991Încă nu există evaluări
- Ameriplan-Health Ameriplan BrochureDocument5 paginiAmeriplan-Health Ameriplan Brochureapi-242298828Încă nu există evaluări
- Advantage Blue: Summary of BenefitsDocument4 paginiAdvantage Blue: Summary of BenefitsDeeDee JonesÎncă nu există evaluări
- Nce Member Handbook Dental ShieldDocument16 paginiNce Member Handbook Dental Shieldapi-304807209Încă nu există evaluări
- Bupa ClassicExtras NSW ACT 0415Document3 paginiBupa ClassicExtras NSW ACT 0415Investor ProtegeÎncă nu există evaluări
- Open Access Plus: Connecticut General Life Insurance Co.: This Is Only A SummaryDocument20 paginiOpen Access Plus: Connecticut General Life Insurance Co.: This Is Only A Summaryswapnil343Încă nu există evaluări
- KP Dcgold020dentalpeddental IvlDocument8 paginiKP Dcgold020dentalpeddental IvlKhamed TabetÎncă nu există evaluări
- MPUSD Benefits SummaryDocument1 paginăMPUSD Benefits SummaryMonterey Peninsula Unified School DistrictÎncă nu există evaluări
- Keep Smiling: Delta Dental PPO™Document2 paginiKeep Smiling: Delta Dental PPO™olimaziÎncă nu există evaluări
- 2016 Employee Benefit Summary For Graduate Assistants, Post-Doctoral Appointees and Short-Term Academic AppointmentsDocument10 pagini2016 Employee Benefit Summary For Graduate Assistants, Post-Doctoral Appointees and Short-Term Academic Appointmentszazoo17Încă nu există evaluări
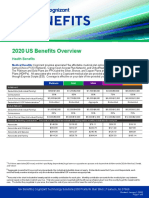
- 2020 US Benefits OverviewDocument5 pagini2020 US Benefits OverviewrdmÎncă nu există evaluări
- Medicare AetnaplanbenefitsDocument22 paginiMedicare AetnaplanbenefitsBert GeorgeÎncă nu există evaluări
- Delta Dental of California - Dental Ppo 12Document2 paginiDelta Dental of California - Dental Ppo 12api-252555369Încă nu există evaluări
- Dental Benefit DetailsDocument3 paginiDental Benefit DetailsFernanda VargasÎncă nu există evaluări
- Young Singles and Couples Product Summary: You Get With HCFDocument4 paginiYoung Singles and Couples Product Summary: You Get With HCFJames SandersÎncă nu există evaluări
- Ins Flex Guideon 17Document1 paginăIns Flex Guideon 17api-97071804Încă nu există evaluări
- BlueDental Copayment QF Plan BrochureDocument4 paginiBlueDental Copayment QF Plan BrochureJoshua JohnsonÎncă nu există evaluări
- PDSB Benefit Plan BookletDocument35 paginiPDSB Benefit Plan BookletDan BouchardÎncă nu există evaluări
- Dental Blue Program 2: (With Orthodontics)Document5 paginiDental Blue Program 2: (With Orthodontics)Cande ArÎncă nu există evaluări
- Budget Hospital and Super Extras Cover: Question? Need Advice? Consultants Available To HelpDocument11 paginiBudget Hospital and Super Extras Cover: Question? Need Advice? Consultants Available To HelpMaik SpaikÎncă nu există evaluări
- DWN HV Brochure 0829Document7 paginiDWN HV Brochure 0829Marquis C Jones Sr.Încă nu există evaluări
- Univ of Chicago PPO Highlights 9-09Document2 paginiUniv of Chicago PPO Highlights 9-09rsheridaÎncă nu există evaluări
- AWANE: Massachusetts PPO 2000: This Is Only A SummaryDocument13 paginiAWANE: Massachusetts PPO 2000: This Is Only A SummaryAutomotive Wholesalers Association of New EnglandÎncă nu există evaluări
- Dental Option 1Document2 paginiDental Option 10pt618Încă nu există evaluări
- Benefits HighlightsDocument1 paginăBenefits HighlightsRobert AvramescuÎncă nu există evaluări
- Dentists: What You Need to Know Before Choosing a DentistDe la EverandDentists: What You Need to Know Before Choosing a DentistÎncă nu există evaluări
- Why Denali Dental and Vision PowerpointDocument15 paginiWhy Denali Dental and Vision PowerpointJohn BerkowitzÎncă nu există evaluări
- LifeLock Presentation - How LifeLock WorksDocument10 paginiLifeLock Presentation - How LifeLock WorksJohn BerkowitzÎncă nu există evaluări
- Denali One Life VisionDocument3 paginiDenali One Life VisionJohn BerkowitzÎncă nu există evaluări
- Direct Vision Insurance Web Site BrochureDocument4 paginiDirect Vision Insurance Web Site BrochureJohn BerkowitzÎncă nu există evaluări
- Direct Vision Insurance BrochureDocument4 paginiDirect Vision Insurance BrochureJohn BerkowitzÎncă nu există evaluări
- Direct Vision Insurance Agent Appointment.Document10 paginiDirect Vision Insurance Agent Appointment.John BerkowitzÎncă nu există evaluări
- Spirit Dental PowerpointDocument21 paginiSpirit Dental PowerpointJohn BerkowitzÎncă nu există evaluări
- Why Denali Dental PowerPoint (Final)Document14 paginiWhy Denali Dental PowerPoint (Final)John BerkowitzÎncă nu există evaluări
- Denalibenefit4pg 0912Document4 paginiDenalibenefit4pg 0912John BerkowitzÎncă nu există evaluări
- Direct Vision Insurance (VSP) CertificateDocument42 paginiDirect Vision Insurance (VSP) CertificateJohn BerkowitzÎncă nu există evaluări
- Why Spirit Dental PowerpointDocument15 paginiWhy Spirit Dental PowerpointJohn BerkowitzÎncă nu există evaluări
- Why Denali Dental PowerPoint (Final)Document14 paginiWhy Denali Dental PowerPoint (Final)John BerkowitzÎncă nu există evaluări
- Why Denali Dental PowerPoint (Final)Document14 paginiWhy Denali Dental PowerPoint (Final)John BerkowitzÎncă nu există evaluări
- Denali Premier Supplemental Agent Appointment 15%Document14 paginiDenali Premier Supplemental Agent Appointment 15%John BerkowitzÎncă nu există evaluări
- IDS701Document26 paginiIDS701Juan Hidalgo100% (2)
- Aperio CS2 BrochureDocument3 paginiAperio CS2 BrochurelailaÎncă nu există evaluări
- 2010 LeftySpeed Oms en 0Document29 pagini2010 LeftySpeed Oms en 0Discord ShadowÎncă nu există evaluări
- Microeconomics Theory and Applications 12th Edition Browning Solutions ManualDocument5 paginiMicroeconomics Theory and Applications 12th Edition Browning Solutions Manualhauesperanzad0ybz100% (26)
- Buckling Analysis of Cylindrical ShellsDocument4 paginiBuckling Analysis of Cylindrical ShellsVPN NetworkÎncă nu există evaluări
- PROCEMAC PT Spare Parts ManualDocument27 paginiPROCEMAC PT Spare Parts ManualMauricio CruzÎncă nu există evaluări
- C# Program To Print Even NumbersDocument11 paginiC# Program To Print Even NumbersNadikattu RavikishoreÎncă nu există evaluări
- 2012 Brochure Keltan Final en PDFDocument20 pagini2012 Brochure Keltan Final en PDFJorge Zegarra100% (1)
- Spark - Eastern Peripheral Road Project (Epr) Weekly Quality MeetingDocument6 paginiSpark - Eastern Peripheral Road Project (Epr) Weekly Quality Meetingengr.s.a.malik6424Încă nu există evaluări
- 03 Marine Multispecies Hatchery Complex Plumbing Detailed BOQ - 23.10.2019Document52 pagini03 Marine Multispecies Hatchery Complex Plumbing Detailed BOQ - 23.10.2019samir bendreÎncă nu există evaluări
- G6Document14 paginiG6Arinah RdhÎncă nu există evaluări
- Tran Date Value Date Tran Particular Credit Debit BalanceDocument96 paginiTran Date Value Date Tran Particular Credit Debit BalanceGenji MaÎncă nu există evaluări
- ExSchutzkatalog Englisch 1Document61 paginiExSchutzkatalog Englisch 1marius_brkt6284Încă nu există evaluări
- Windows XP, Vista, 7, 8, 10 MSDN Download (Untouched)Document5 paginiWindows XP, Vista, 7, 8, 10 MSDN Download (Untouched)Sheen QuintoÎncă nu există evaluări
- Hydrostatic Pressure Test Safety ChecklistDocument3 paginiHydrostatic Pressure Test Safety ChecklistJerry Faria60% (5)
- 48 - 1997 SummerDocument42 pagini48 - 1997 SummerLinda ZwaneÎncă nu există evaluări
- Rosmary PollockDocument4 paginiRosmary PollockhbÎncă nu există evaluări
- Zambia Urban Housing Sector ProfileDocument205 paginiZambia Urban Housing Sector ProfileJosephine ChirwaÎncă nu există evaluări
- 8 e Daft Chapter 01Document29 pagini8 e Daft Chapter 01GabÎncă nu există evaluări
- HP Mini 210-2120br PC Broadcom Wireless LAN Driver v.5.60.350.23 Pour Windows 7 Download GrátisDocument5 paginiHP Mini 210-2120br PC Broadcom Wireless LAN Driver v.5.60.350.23 Pour Windows 7 Download GrátisFernandoDiasÎncă nu există evaluări
- INCOME TAX AND GST. JURAZ-Module 4Document8 paginiINCOME TAX AND GST. JURAZ-Module 4TERZO IncÎncă nu există evaluări
- Test P1 Chapter 10Document10 paginiTest P1 Chapter 10Prince PersiaÎncă nu există evaluări
- 1ST Term S1 Physics-1Document33 pagini1ST Term S1 Physics-1onos arereÎncă nu există evaluări
- Life Lessons AssignmentDocument5 paginiLife Lessons Assignmentapi-332560669Încă nu există evaluări
- New CVLRDocument2 paginiNew CVLRanahata2014Încă nu există evaluări
- LeasesDocument9 paginiLeasesCris Joy BiabasÎncă nu există evaluări
- MSSQL and Devops DumpsDocument5 paginiMSSQL and Devops DumpsRishav GuptaÎncă nu există evaluări