S-ar putea să vă placă și
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideDe la EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideÎncă nu există evaluări
- ABGs Respiratory/MetabolicDocument3 paginiABGs Respiratory/MetabolicJoe B100% (1)
- Arterial Blood Gas Analysis - making it easyDe la EverandArterial Blood Gas Analysis - making it easyEvaluare: 4.5 din 5 stele4.5/5 (4)
- Blood Gas InterpretationDocument36 paginiBlood Gas InterpretationMary Charmaine DivinagraciaÎncă nu există evaluări
- Fluid and Electrolytes for Nursing StudentsDe la EverandFluid and Electrolytes for Nursing StudentsEvaluare: 5 din 5 stele5/5 (12)
- ABG Interpretation - ATSDocument5 paginiABG Interpretation - ATSHAMMYER ALROKHAMIÎncă nu există evaluări
- Respiratory Acidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandRespiratory Acidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Icu Nurse SheetDocument1 paginăIcu Nurse SheetJan MarcusÎncă nu există evaluări
- Nursing Care of PlanDocument16 paginiNursing Care of PlanDbyÎncă nu există evaluări
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsDe la EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsÎncă nu există evaluări
- ABG Practice Problems For N304Document4 paginiABG Practice Problems For N304dlneisha61100% (2)
- Dimensional Analysis For Nursing StudentsDe la EverandDimensional Analysis For Nursing StudentsÎncă nu există evaluări
- EKG Basics1Document16 paginiEKG Basics1Jamie Lemons100% (1)
- 14 Fun Facts About Your Heart: Educational VersionDe la Everand14 Fun Facts About Your Heart: Educational VersionÎncă nu există evaluări
- Cardiac Med ChartsDocument6 paginiCardiac Med ChartsNursingSchoolNotes100% (15)
- Schaum's Outline of Critical Care Nursing: 250 Review QuestionsDe la EverandSchaum's Outline of Critical Care Nursing: 250 Review QuestionsEvaluare: 5 din 5 stele5/5 (1)
- Shock Comparison ChartDocument2 paginiShock Comparison Chartlinnaete88% (8)
- CRITICAL CARE NURSE: Passbooks Study GuideDe la EverandCRITICAL CARE NURSE: Passbooks Study GuideÎncă nu există evaluări
- Respiratory PathophysDocument1 paginăRespiratory PathophysTori IkeharaÎncă nu există evaluări
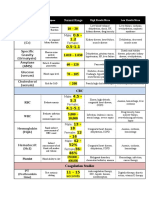
- Lab ValuesDocument3 paginiLab Valuessurviving nursing school100% (1)
- Understanding ElectrolytesDocument2 paginiUnderstanding Electrolytessurviving nursing schoolÎncă nu există evaluări
- Heart FailureDocument1 paginăHeart FailureTrisha Vergara100% (1)
- Acid Base Who Is Your DaddyDocument66 paginiAcid Base Who Is Your Daddyjenn1722100% (14)
- Critical Care NursingDocument1 paginăCritical Care NursingMelissa David0% (1)
- ICU Cheat SheetDocument2 paginiICU Cheat SheetPrescilla Randazzo100% (1)
- ABG InterpretationDocument31 paginiABG Interpretationɹǝʍdןnos100% (12)
- My Cheat SheetDocument3 paginiMy Cheat SheetTenzin KyizomÎncă nu există evaluări
- Cardiac Study GuideDocument11 paginiCardiac Study Guidejenwiley318096% (73)
- Shock Study Guide NursingDocument4 paginiShock Study Guide NursingKory Christina100% (2)
- EKG Quick Reference ChartDocument4 paginiEKG Quick Reference ChartMildaÎncă nu există evaluări
- Acid-Base WorksheetDocument2 paginiAcid-Base WorksheetMayer Rosenberg100% (18)
- Arterial Blood Gases Made Easy PDFDocument66 paginiArterial Blood Gases Made Easy PDFTamjid Khan100% (5)
- Nursing Patho CardsDocument195 paginiNursing Patho Cardsgiogmail100% (1)
- Simple Method of Acid Base Balance Interpretation: UsefulnessDocument2 paginiSimple Method of Acid Base Balance Interpretation: UsefulnessPeej ReyesÎncă nu există evaluări
- ABG Made EasyDocument10 paginiABG Made EasyMayer Rosenberg100% (38)
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDocument3 paginiDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- Arterial Lines in PACU: Presented by Autum Jacobs RN, BSNDocument34 paginiArterial Lines in PACU: Presented by Autum Jacobs RN, BSNinuko1212Încă nu există evaluări
- Med Surg Respiration-Cardiac NotesDocument11 paginiMed Surg Respiration-Cardiac Notesorganictallgirl50% (2)
- Acuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiesDocument16 paginiAcuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiessamuelÎncă nu există evaluări
- Alkalosis Acidosis ChartDocument1 paginăAlkalosis Acidosis ChartrobingailÎncă nu există evaluări
- Management of Mechanical VentilationDocument16 paginiManagement of Mechanical Ventilationyuliana muinÎncă nu există evaluări
- Arterial LinesDocument13 paginiArterial LinesberhanubedassaÎncă nu există evaluări
- Med Surg Cheat Sheet 1Document1 paginăMed Surg Cheat Sheet 1Figmentum FigmentumÎncă nu există evaluări
- Abg InterpretationDocument14 paginiAbg Interpretationmara5140100% (7)
- Sample Acls For DummiesDocument3 paginiSample Acls For DummiesTodd Cole100% (1)
- Approach To The Patient With Respiratory DiseaseDocument6 paginiApproach To The Patient With Respiratory DiseaseRem AlfelorÎncă nu există evaluări
- Critical CareDocument40 paginiCritical Carenkuligowski100% (6)
- Abg Made EasyDocument24 paginiAbg Made EasynbvillarazoÎncă nu există evaluări
- Ams 11Document702 paginiAms 11CrazyÎncă nu există evaluări
- Ecgs Made Easy 5th Edition Aehlert Test BankDocument14 paginiEcgs Made Easy 5th Edition Aehlert Test BankQuinn50% (2)
- Practice StripsDocument9 paginiPractice StripsErica Yamamoto50% (4)
- Arterial Blood GasesDocument44 paginiArterial Blood GasesRidhwan Mgt100% (1)
- Sepsis, Septic Shock, MODSDocument19 paginiSepsis, Septic Shock, MODSPaul Zantua80% (5)
- MedicalSurgical Nursing ReviewDocument86 paginiMedicalSurgical Nursing ReviewPopa D. SilviuÎncă nu există evaluări
- ACAQ Crit Care Nursing CurriculumDocument91 paginiACAQ Crit Care Nursing CurriculumAnne Julia Agustin100% (1)
- Vent Modes ChartDocument1 paginăVent Modes Chartladyhavocinc100% (1)
- Cardiac Meds ChartDocument1 paginăCardiac Meds ChartCharlotte Louise75% (4)
- ABG AnalysisDocument22 paginiABG Analysisrajan40dmcÎncă nu există evaluări
- Pathophysiology of Respiratory DiseasesDocument8 paginiPathophysiology of Respiratory DiseasesTONY GO AWAYÎncă nu există evaluări
- Catedral de SevillaDocument28 paginiCatedral de SevillaAnonymous LkgNmKeÎncă nu există evaluări
- Cambridge IGCSE™: Information and Communication Technology 0417/13 May/June 2022Document15 paginiCambridge IGCSE™: Information and Communication Technology 0417/13 May/June 2022ilovefettuccineÎncă nu există evaluări
- Sociology As A Form of Consciousness - 20231206 - 013840 - 0000Document4 paginiSociology As A Form of Consciousness - 20231206 - 013840 - 0000Gargi sharmaÎncă nu există evaluări
- SOL LogicDocument21 paginiSOL LogicJa RiveraÎncă nu există evaluări
- Development Developmental Biology EmbryologyDocument6 paginiDevelopment Developmental Biology EmbryologyBiju ThomasÎncă nu există evaluări
- Micro EvolutionDocument9 paginiMicro EvolutionBryan TanÎncă nu există evaluări
- Listen and Arrange The Sentences Based On What You Have Heard!Document3 paginiListen and Arrange The Sentences Based On What You Have Heard!Dewi Hauri Naura HaufanhazzaÎncă nu există evaluări
- Thesis PaperDocument53 paginiThesis PaperAnonymous AOOrehGZAS100% (1)
- Lesson 6 - Vibration ControlDocument62 paginiLesson 6 - Vibration ControlIzzat IkramÎncă nu există evaluări
- Lecture2 GranulopoiesisDocument9 paginiLecture2 GranulopoiesisAfifa Prima GittaÎncă nu există evaluări
- Leadership Styles-Mckinsey EdDocument14 paginiLeadership Styles-Mckinsey EdcrimsengreenÎncă nu există evaluări
- Unsuccessful MT-SM DeliveryDocument2 paginiUnsuccessful MT-SM DeliveryPitam MaitiÎncă nu există evaluări
- Workbook Group TheoryDocument62 paginiWorkbook Group TheoryLi NguyenÎncă nu există evaluări
- Hidrl1 PDFDocument7 paginiHidrl1 PDFRajesh Kumar100% (1)
- DLP - Light Science 7Document6 paginiDLP - Light Science 7Samara M. SalacayanÎncă nu există evaluări
- Amount of Casien in Diff Samples of Milk (U)Document15 paginiAmount of Casien in Diff Samples of Milk (U)VijayÎncă nu există evaluări
- Fire Protection in BuildingsDocument2 paginiFire Protection in BuildingsJames Carl AriesÎncă nu există evaluări
- Sem4 Complete FileDocument42 paginiSem4 Complete Fileghufra baqiÎncă nu există evaluări
- Biblical World ViewDocument15 paginiBiblical World ViewHARI KRISHAN PALÎncă nu există evaluări
- What's New in CAESAR II: Piping and Equipment CodesDocument1 paginăWhat's New in CAESAR II: Piping and Equipment CodeslnacerÎncă nu există evaluări
- 6GK74435DX040XE0 Datasheet enDocument3 pagini6GK74435DX040XE0 Datasheet enLuis CortezÎncă nu există evaluări
- Baseline Scheduling Basics - Part-1Document48 paginiBaseline Scheduling Basics - Part-1Perwaiz100% (1)
- ECE Companies ListDocument9 paginiECE Companies ListPolaiah Geriki100% (1)
- The RBG Blueprint For Black Power Study Cell GuidebookDocument8 paginiThe RBG Blueprint For Black Power Study Cell GuidebookAra SparkmanÎncă nu există evaluări
- Executive Summary-P-5 181.450 To 222Document14 paginiExecutive Summary-P-5 181.450 To 222sat palÎncă nu există evaluări
- Contents EEMUA Publication 190 Edition1 May 2015Document4 paginiContents EEMUA Publication 190 Edition1 May 2015Aditya JainÎncă nu există evaluări
- Lecture 14 Direct Digital ManufacturingDocument27 paginiLecture 14 Direct Digital Manufacturingshanur begulaji0% (1)
- Inside:: Issue 4 - February 2004 Bi-Monthly Warhammer E-ZineDocument40 paginiInside:: Issue 4 - February 2004 Bi-Monthly Warhammer E-ZineJoe BloggsÎncă nu există evaluări
- Activity Title: Learning Targets: Reference (S)Document5 paginiActivity Title: Learning Targets: Reference (S)Jhev LeopandoÎncă nu există evaluări
- Triaxial Shear TestDocument10 paginiTriaxial Shear TestAfiqah Nu'aimiÎncă nu există evaluări