S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- 2012 SLICC Criteria Systemic Lupus ErythematosusDocument10 pagini2012 SLICC Criteria Systemic Lupus ErythematosusNaufal AndaluÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Intussusception: PathophysiologyDocument8 paginiIntussusception: PathophysiologyNaufal AndaluÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Pandrug-Resistant Causing Nosocomial Infections in A University Hospital, TaiwanDocument6 paginiPandrug-Resistant Causing Nosocomial Infections in A University Hospital, TaiwanNaufal AndaluÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Central Line - Associated Bloodstream Infections: Anthony J. Baldea, JR., MD, and Christine S. Cocanour, MD, FACS, FCCMDocument4 paginiCentral Line - Associated Bloodstream Infections: Anthony J. Baldea, JR., MD, and Christine S. Cocanour, MD, FACS, FCCMNaufal AndaluÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Impact of Smoking and Smoking Cessation On Overweight and Obesity: Scotland-Wide, Cross-Sectional Study On 40,036 ParticipantsDocument8 paginiImpact of Smoking and Smoking Cessation On Overweight and Obesity: Scotland-Wide, Cross-Sectional Study On 40,036 ParticipantsNaufal AndaluÎncă nu există evaluări
- Nurses Germany enDocument131 paginiNurses Germany enwkkevinnÎncă nu există evaluări
- ThiruvananthapuramDocument31 paginiThiruvananthapuramsuryadev s24Încă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoku AnafilaktikDocument16 paginiShoku AnafilaktikindeenikeÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- nRICH Article 31Document6 pagininRICH Article 31sanjeev kumarÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Uechi RyuDocument13 paginiUechi RyualexnadaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- A Guide For Monitoring Child Development in Low - and Middle-Income CountriesDocument11 paginiA Guide For Monitoring Child Development in Low - and Middle-Income Countriesanisetiyowati14230% (1)
- Sinus Lift ChenDocument10 paginiSinus Lift ChenCarlos Frederico Nunes PavãoÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Secret of Being HappyDocument282 paginiThe Secret of Being Happylcs1234678100% (3)
- Immediate Care Competency (Baby Care)Document3 paginiImmediate Care Competency (Baby Care)Louie Jay Ramos100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Nepal Health Professional Council: Syllabus For Licensing Examination of Certificate in Physiotherapy 2021Document4 paginiNepal Health Professional Council: Syllabus For Licensing Examination of Certificate in Physiotherapy 2021HariÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Jurnal Diare RotavirusDocument6 paginiJurnal Diare RotavirusAnhi RamdhaniÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Electric Hot Water Bag IncidentDocument2 paginiElectric Hot Water Bag IncidentKmt_AeÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Health Care Delivery System AT National, State, District & Local LevelDocument92 paginiHealth Care Delivery System AT National, State, District & Local Levelangayarkanni100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Prophylactic Use of Fluconazole in Very Premature InfantsDocument7 paginiProphylactic Use of Fluconazole in Very Premature InfantsYurika Elizabeth SusantiÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
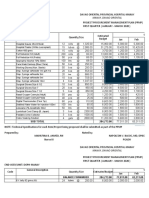
- PPMP Medical Supplies 2020Document16 paginiPPMP Medical Supplies 2020Jan Oneille Y. VallesÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Neonatal TransportDocument35 paginiNeonatal TransportBhupendra GuptaÎncă nu există evaluări
- LorazepamDocument14 paginiLorazepamJuan PerezÎncă nu există evaluări
- Daftar Pustaka BPSDDocument2 paginiDaftar Pustaka BPSDEffendy ZhuoÎncă nu există evaluări
- Rehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureDocument4 paginiRehabilitation Exercises To Induce Balanced Scapular Muscle Activity in An Anti-Gravity PostureSAMÎncă nu există evaluări
- Lamaze Seperatingmomandbabyinfographic Final 1Document1 paginăLamaze Seperatingmomandbabyinfographic Final 1api-264859193Încă nu există evaluări
- CAMERON Current Surgical Therapy, Thirteenth EditionDocument1.667 paginiCAMERON Current Surgical Therapy, Thirteenth Editionniberev100% (2)
- ALERT Adverse Late Effects of Cancer Treatment Volume 2Document710 paginiALERT Adverse Late Effects of Cancer Treatment Volume 2Cosmin SaftaÎncă nu există evaluări
- Oxford Handbook of Anaesthesia (Rachel Freedman, Lara Herbert Etc.)Document1.273 paginiOxford Handbook of Anaesthesia (Rachel Freedman, Lara Herbert Etc.)Liana Naamneh100% (2)
- Molnar CPDocument4 paginiMolnar CPCatherine AgustinÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Company ProfileDocument5 paginiCompany ProfileHai HelloÎncă nu există evaluări
- Sassouni AnalisisDocument2 paginiSassouni Analisisナスティオン ファジャルÎncă nu există evaluări
- Callens Ultrasonography in 181103190514Document5 paginiCallens Ultrasonography in 181103190514dr.Rizna Ariyani0% (4)
- Medscape Status EpilepticusDocument10 paginiMedscape Status EpilepticusEllen Siska SusantiÎncă nu există evaluări
- Fma Ue EnglishDocument3 paginiFma Ue EnglishAnaa ElleyÎncă nu există evaluări
- GE Dinamap Pro 1000 - Service ManualDocument109 paginiGE Dinamap Pro 1000 - Service Manualpatrick1009Încă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)