S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Common HCC Codes and Diabetes Manifestations SheetDocument2 paginiCommon HCC Codes and Diabetes Manifestations SheetmeikaizenÎncă nu există evaluări
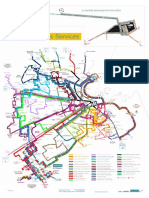
- Mowasalat Bus RouteDocument1 paginăMowasalat Bus Routeshabina92129% (7)
- Question: 1 of 100 / Overall Score: 80%: True / FalseDocument84 paginiQuestion: 1 of 100 / Overall Score: 80%: True / FalseGalaleldin AliÎncă nu există evaluări
- Herbs or Natural Products CancerDocument16 paginiHerbs or Natural Products CancerANGELO NHAR100% (1)
- Nurs208 K4yDocument12 paginiNurs208 K4yapi-347145789100% (2)
- Ananth Narayan and Paniker 11th EditionDocument42 paginiAnanth Narayan and Paniker 11th EditionArjun Kandara50% (2)
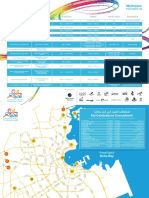
- Eid Celebrations in Qatar 2016 - Schedule & MapDocument2 paginiEid Celebrations in Qatar 2016 - Schedule & Mapshabina921Încă nu există evaluări
- Sports Village ScheduleDocument5 paginiSports Village Scheduleshabina921Încă nu există evaluări
- The U.S. State Department Removed Cuba and Malaysia From Its Human Trafficking BlacklistDocument384 paginiThe U.S. State Department Removed Cuba and Malaysia From Its Human Trafficking BlacklistBarbara EspinosaÎncă nu există evaluări
- MasterCard Muslim IndexDocument38 paginiMasterCard Muslim IndexshinkoicagmailcomÎncă nu există evaluări
- WEF Human Capital Report 2015 - QatarDocument2 paginiWEF Human Capital Report 2015 - Qatarshabina921Încă nu există evaluări
- Bayt Job Satisfaction Report 04 2015Document62 paginiBayt Job Satisfaction Report 04 2015shabina921Încă nu există evaluări
- Home Rental Rates and Affordability in QatarDocument12 paginiHome Rental Rates and Affordability in Qatarshabina921Încă nu există evaluări
- October Statistics - Ministry of Development, Planning and StatisticsDocument24 paginiOctober Statistics - Ministry of Development, Planning and Statisticsshabina921Încă nu există evaluări
- CPI BrochureDocument12 paginiCPI BrochureRashi MathurÎncă nu există evaluări
- Katara National Day Activities 2014Document3 paginiKatara National Day Activities 2014shabina921Încă nu există evaluări
- Children and Women ReportDocument236 paginiChildren and Women Reportshabina921Încă nu există evaluări
- KamranDocument1 paginăKamranshabina921Încă nu există evaluări
- Qatar Monthly Statistics Edition 8 For Web 2Document21 paginiQatar Monthly Statistics Edition 8 For Web 2shabina921Încă nu există evaluări
- Qatar Monthly Statistics August 2014 Edition 7Document22 paginiQatar Monthly Statistics August 2014 Edition 7shabina921Încă nu există evaluări
- Qatar Tourism Authority Mall Entertainment ScheduleDocument1 paginăQatar Tourism Authority Mall Entertainment Scheduleshabina921Încă nu există evaluări
- FIFA Ethics StatementDocument42 paginiFIFA Ethics Statementshabina921Încă nu există evaluări
- InterNations Survey Report Top Expat Destinations 2014 PDFDocument197 paginiInterNations Survey Report Top Expat Destinations 2014 PDFcaidas_libresÎncă nu există evaluări
- WWF Living Planet Report 2014Document180 paginiWWF Living Planet Report 2014ishmael daroÎncă nu există evaluări
- 2014 Human Development Report English PDFDocument239 pagini2014 Human Development Report English PDFMiguel BenedettiÎncă nu există evaluări
- Qatar Monthly Statistics July 2014 Edition 6Document22 paginiQatar Monthly Statistics July 2014 Edition 6shabina921Încă nu există evaluări
- Qatar Monthly Statistics July 2014 Edition 6Document22 paginiQatar Monthly Statistics July 2014 Edition 6shabina921Încă nu există evaluări
- CITES Cheetah ReportDocument54 paginiCITES Cheetah Reportshabina921Încă nu există evaluări
- GCC Education Industry Report July 2014Document97 paginiGCC Education Industry Report July 2014shabina921Încă nu există evaluări
- EN Draft E-Participation PolicyDocument59 paginiEN Draft E-Participation Policyshabina921Încă nu există evaluări
- Household Expenditure EngDocument206 paginiHousehold Expenditure Engshabina921Încă nu există evaluări
- Migrant Labour Recruitment To QatarDocument162 paginiMigrant Labour Recruitment To Qatarshabina921100% (1)
- Capital Projects Survey 2014Document28 paginiCapital Projects Survey 2014shabina921Încă nu există evaluări
- Qatar Monthly Statistics Edition 5 For PrintDocument24 paginiQatar Monthly Statistics Edition 5 For Printshabina921Încă nu există evaluări
- Colorectal Disease - 2023 - Suarez Pazos - Step by Step Surgical Technique For Robotic Kono S Anastomosis After Small BowelDocument2 paginiColorectal Disease - 2023 - Suarez Pazos - Step by Step Surgical Technique For Robotic Kono S Anastomosis After Small BowelCLINIC SURGERY 17THÎncă nu există evaluări
- D5LRDocument2 paginiD5LRLouiseville Ann Arcilla PilÎncă nu există evaluări
- BupropionDocument3 paginiBupropionRJ HÎncă nu există evaluări
- 13 BDocument38 pagini13 BBruno100% (4)
- Milk Ring TestDocument25 paginiMilk Ring TestDilhan Anuradha Wimalaratne71% (7)
- Urinalysis Control - Level 2 (Urnal Control 2) : Cat. No. UC5034 Lot No. 737UC Size: Expiry: 2015-10Document6 paginiUrinalysis Control - Level 2 (Urnal Control 2) : Cat. No. UC5034 Lot No. 737UC Size: Expiry: 2015-10Meiliana ThanÎncă nu există evaluări
- New School Health FormsDocument42 paginiNew School Health FormsJoanna MarieÎncă nu există evaluări
- Golongan ObatDocument29 paginiGolongan ObatMala PanoÎncă nu există evaluări
- Solution Manual For Understanding The Essentials of Critical Care Nursing 2nd Edition by PerrinDocument15 paginiSolution Manual For Understanding The Essentials of Critical Care Nursing 2nd Edition by PerrinMarieHughesebgjp100% (75)
- Physical Therapy Modalities and Rehabilitation Techniques in The Treatment of Neuropathic Pain jpmr.1000124 PDFDocument4 paginiPhysical Therapy Modalities and Rehabilitation Techniques in The Treatment of Neuropathic Pain jpmr.1000124 PDFvinika ChaudharyÎncă nu există evaluări
- 2018 AHA Guidelines For Management of Blood CholesterolDocument66 pagini2018 AHA Guidelines For Management of Blood CholesterolsarumaxÎncă nu există evaluări
- Annotated BibliographyDocument5 paginiAnnotated Bibliographyapi-286443025Încă nu există evaluări
- PolytraumaDocument41 paginiPolytraumaFrederick Mars UntalanÎncă nu există evaluări
- ABC Bone CystDocument43 paginiABC Bone CystIrfan Ullah KhanÎncă nu există evaluări
- Biochemistry: Inside The LabDocument1 paginăBiochemistry: Inside The LabAsim aliÎncă nu există evaluări
- X Ray ProtocolDocument2 paginiX Ray ProtocolKhaidir AlimÎncă nu există evaluări
- Contractura 11 PDFDocument2 paginiContractura 11 PDFVillateAngelaÎncă nu există evaluări
- KodingDocument12 paginiKodingAva Vav100% (1)
- New York Imaging Specialists Announces Grand Opening in Port Jefferson StationDocument2 paginiNew York Imaging Specialists Announces Grand Opening in Port Jefferson StationPR.comÎncă nu există evaluări
- Second Medical Use CountriesDocument5 paginiSecond Medical Use CountriesAnonymous AWcEiTj5u0Încă nu există evaluări
- Public Health Microbiology - 4th EdDocument39 paginiPublic Health Microbiology - 4th EdaphethuxolomÎncă nu există evaluări
- Nab-Paclitaxel Mechanisms of Action and Delivery 2013Document8 paginiNab-Paclitaxel Mechanisms of Action and Delivery 2013Tamara Chachi-Baía do SantiagoÎncă nu există evaluări
- Spotting Signs of AutismDocument23 paginiSpotting Signs of AutismAutism Parenting100% (3)
- CVA Impaired Physical MobilityDocument2 paginiCVA Impaired Physical MobilitycessyanneÎncă nu există evaluări
- Sample Questions For HAAD Prometric and DHA For NursesDocument46 paginiSample Questions For HAAD Prometric and DHA For NursesJaezelle Ella Sabale100% (4)