Documente Academic
Documente Profesional
Documente Cultură
1 s2.0 S000293781100072X Main
Încărcat de
Joa LizDescriere originală:
Titlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
1 s2.0 S000293781100072X Main
Încărcat de
Joa LizDrepturi de autor:
Formate disponibile
Research
www. AJOG.org
ONCOLOGY
Treating cervical cancer: Breast and Cervical Cancer
Prevention and Treatment Act patients
Li-Nien Chien, PhD; E. Kathleen Adams, PhD; Lisa C. Flowers, MD
OBJECTIVE: To investigate cervical cancer treatment of patients en-
rolled under the Breast and Cervical Cancer Prevention and Treatment
Act in Georgia.
STUDY DESIGN: Georgia Comprehensive Cancer Registry and Medicaid enrollment/claims were used to identify enrollees with preinvasive
disease (n 1149) and invasive cervical cancer (n 444). Logistic
regressions were used to estimate factors associated with the odds of
receiving: (1) cancer workup, (2) precancerous procedure, (3) surgery,
(4) radiation, and (5) chemotherapy.
proved hospital nearby were more likely to receive surgery. Among invasive cases, later stage was associated with higher odds of receiving
radiation or chemotherapy. Black patients were less likely to have surgery than white patients regardless of preinvasive (P .01) or invasive
status (P .05).
CONCLUSION: Treatment patterns among Georgia Medicaid cases ap-
pear appropriate to stage but 18% with invasive cervical cancer received no cancer treatment, although Medicaid enrolled.
RESULTS: Preinvasive disease cases with cervical intraepithelial neo-
plasia 3, in situ, a comorbidity or without a Commission on Cancer ap-
Key words: BCCPTA, cancer treatment, cervical cancer, Medicaid
Cite this article as: Chien L-N, Adams EK, Flowers LC. Treating cervical cancer: Breast and Cervical Cancer Prevention and Treatment Act patients. Am J Obstet
Gynecol 2011;204:533.e1-8.
ervical cancer is one of the most
common female cancers in the
United States. The American Cancer
Society (ACS) estimates approximately
11,270 new cases will be diagnosed with
invasive cervical cancer and that there
will be 4070 related deaths in 2009.1 The
incidence and mortality of invasive cervical cancer has declined dramatically
since the mid 1940s because of the wide
use of Papanicolaou (Pap) smear and
early detection and treatment of cervical
intraepithelial neoplasia (CIN).2-4 However, this disease is not evenly distributed
across segments of the US population.
Women who were low income,5 low education, or uninsured6 were more likely to
have a higher incidence and mortality
From the Department of Health Policy and
Management (Drs Chien and Adams),
Rollins School of Public Health, and the
Department of Gynecology and Obstetrics
(Dr Flowers), Emory University, Atlanta,
GA.
Reprints not available from the authors.
Supported by Grant no. RSGT-05-004-01CPHPS from the American Cancer Society.
0002-9378/$36.00
2011 Mosby, Inc. All rights reserved.
doi: 10.1016/j.ajog.2011.01.033
mainly because of failure to detect and
treat the cancer early.7-13 Unlike the patterns for invasive cervical cancer, the number of cases of CIN has continuously increased, especially in young women.14-16
Two important pieces of legislation
created greater access to cancer screening, diagnosis, and treatment of this
preventable and curable disease. The
National Breast and Cervical Cancer
Early Detection Program (NBCCEDP)
funded by the Centers for Diseases Control
and Prevention, has provided screening
and diagnostic follow-up for low-income
uninsured women since 1990.17 In program year 2008, NBCCEDP screened
301,209 women for breast cancer with
mammography and found 3782 cases of
this disease, whereas also screening
321,296 women for cervical cancer and
detecting 5201 cancers and high-grade
precancerous lesions.18 Research has indicated that the aging of NBCCEDP significantly improved screening rates of
mammography, breast clinic examination, and Pap smear in the late 1990s19
and yet, because of low funding, this program can reach only an estimated 1215% of those eligible.20
Because of the NBCCEDP does not
cover cancer treatment costs,21 Congress
passed the Breast and Cervical Cancer Prevention and Treatment Act (BCCPTA) in
2000 to give states the option of offering
women in the NBCCEDP access to treatment through a special Medicaid coverage.22 BCCPTA was adopted quickly by all
50 states, and Georgia began enrolling
their patients into the Womens Health
Medicaid Program (WHMP) in July
2001. Although BCCPTA mandated that
women be screened by the NBCCEDP,
states had options to extend eligibility to
women screened by non-NBCCEDP providers. Georgia is 1 of 12 states that selected
this more expansive screening option. In
2005, only 25% of BCCPTA women were
screened in health departments through
Georgias NBCCEDP screening program
(known as Breast Test and More); the
majority (75%) of them were screened by
private providers.23 Women will be continuously eligible for BCCPTA as long as
they are considered under cancer treatment by their physicians, although states
differ in their redetermination process. In
2003, BCCPTA women in Georgia could
simply self-report to WHMP every 6
months indicating they were in active
treatment.23
Our earlier work found that BCCPTA
implementation in Georgia led to an in-
JUNE 2011 American Journal of Obstetrics & Gynecology
533.e1
Research
Oncology
crease of 2-3 more women with these
cancers enrolling in Medicaid in a given
month and also shortened the enrollment process by 7-8 months.24 Hence,
breast cancer patients can enroll and potentially, start treatment while still at an
early stage of disease (data unavailable).
This could, in turn, lead to better outcomes and longer survival. The simpler
recertification process under BCCPTA
also created both a stable insurance coverage and connection with the participants health care providers, resulting in
a 50% decline in the rates of disenrollment from Medicaid for both cancers
post-BCCPTA.25
The ultimate goal of BCCPTA is to
provide Medicaid coverage to assure
quality treatment. In Georgia, BCCPTA
breast cancer patients were more likely
to receive any cancer treatment within 2
years of Medicaid enrollment than those
under other Medicaid eligibility groups
(data unavailable). Though there was no
difference in receiving lumpectomy vs
mastectomy; BCCPTA women were
more likely than other groups to receive
adjuvant therapy after surgery. Given the
findings for breast cancer patients, it is
important to understand the cancer
treatment pattern of patients diagnosed
with preinvasive disease and invasive
cervical cancer under BCCPTA.
M ATERIALS AND M ETHODS
Institutional review board
This study was granted Institutional Review Board by the Georgia State Institutional Review Board, the American Cancer Society and Emory University.
Data sources
The major datasets used were the Georgia Cancer Comprehensive Registry
(GCCR), Medicaid enrollment, and
claims files. The GCCR is a state-wide
population-based cancer registry that
collects all cancer cases diagnosed in
Georgia since 1999. Medicaid enrollment files offer monthly eligibility records and Medicaid claims files contain
diagnostic and procedure information
coded by the International Classification
of Disease, 9th Revision, Clinical Modification (ICD-9-CM) and Current Pro533.e2
www.AJOG.org
cedural Terminology (CPT) schema for
medical billing.
The county data were from Area Resource File (ARF), Commission on Cancer (CoC), and Consolidated Analysis
Center, Incorporated (CACI). The ARF,
assembled by the Health Resources and
Services Administration, provides a variety of county-level data for the 159 counties in Georgia. The CoC, established by
the American College of Surgeons, provides data on hospitals that are able to
comply with established CoC standards26 to deliver cancer care. The CACI
US Marketing Systems Group provides
data on households income level at the
county level.27
Study sample
Incident cervical cancer cases in the
GCCR between July 1, 2001, and Dec. 31,
2004, were linked to the Medicaid enrollment file using the patients encrypted
social security number for those identified with a primary site of cancer of cervix (local stage and beyond) (n 470).
We excluded those who enrolled in Medicaid more than 6 months after being diagnosed based on the assumption that
they did not require Medicaid for cancer
treatment on diagnosis (n 25). We
note that the GCCR did not include preinvasive (CIN 2 and 3, in situ) cervical
cases; therefore, we identified those cases
as women who were ever enrolled under
the BCCPTA eligibility category and
were not invasive cervical or breast cancer cases in the GCCR (n 1539).
Of the remaining sample (n 1984),
we excluded those who had more than 1
primary cancer site because their cancer
treatment can be affected by other cancers. To ensure that all women can be
followed for at least for 2 years, we excluded those over 63 years because their
medical claims converted to Medicare at
age 65. Those not continuously enrolled
in Medicaid in the first 2 months were
also excluded because they might not actually be eligible for Medicaid but,
rather, were given presumptive eligibility. The final sample was 1937 patients
covered by Medicaid, 1149 of whom
were diagnosed with preinvasive disease,
444 of whom were diagnosed with invasive cervical cancer and 344 of whom we
American Journal of Obstetrics & Gynecology JUNE 2011
were unable to identify their stage either
from GCCR or Medicaid claims. We
omitted them in later analyses.
Cervical cancer treatment
In conjunction with the treatment guidelines of the National Cancer Institute,28
we examined cervical cancer treatment
as the receipt of any: (1) cancer workup,
(2) precancerous procedure, (3) surgery, (4) radiation, or (5) chemotherapy
among patients with preinvasive and invasive cervical disease.
Cancer workup was defined as a series
of tests and procedures that were needed
to establish the diagnosis to prepare
treatment plans. The standard treatments for patients with preinvasive disease included loop electrosurgical excision procedure (LEEP) and conization,
and simple hysterectomy. Invasive surgery, radiation, and/or chemotherapy
were treatment options for invasive
cases. All treatments were identified
from ICD-9-CM code or CPT codes
contained in the Medicaid claims files.
Study variables
We included patients demographics,
disease conditions, Medicaid enrollment
status, and resident county characteristics to examine factors associated with
the receipt of treatment. Patients covariates included: (1) age at enrollment,
(2) race/ethnicity, (3) stage at diagnosis,
(4) comorbidity index, (5) preenrolled
in Medicaid, (6) Medicaid eligibility
category, and (7) length of Medicaid
enrollment.
The stage data were from either GCCR
or based on Medicaid claims for services
received in or after their month of enrollment. The stage system we used here is
the Surveillance, Epidemiology, and End
Results (SEER) Program summary stage,
which can group cases into 5 main categories: (1) in situ, (2) local, (3) regional,
(4) distant, and (5) unstaged. It can also
be derived from the ICD-9-CM codes in
medical claims, which helps us identify
stage for those not from the GCCR. The
full list of codes for identifying cervical
cancer stage from the claims is available
on request.
To adjust the severity of a noncancer
medical illness, which might affect the
Oncology
www.AJOG.org
Research
TABLE 1
Summary of characteristics of Medicaid enrollees diagnosed with preinvasive and invasive cervical cancer
Classification, %
Variable
Preinvasive (n 1149)
Invasive (n 444)
Age at enrollment, mean (SD)
29.1 (9.6)
42.6 (10.5)
Unstaged (n 344)
Total
34.3 (12.1)
33.1 (11.7)
.......................................................................................................................................................................................................................................................................................................................................................................
19-24
41.7
4.5
27.6
30.7
25-34
34.3
19.1
29.7
30.0
35-44
15.8
33.6
20.1
20.6
45-63
8.3
42.8
22.7
18.7
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................................................................................
Race/Ethnicity
.......................................................................................................................................................................................................................................................................................................................................................................
Non-Hispanic white
66.8
54.7
62.8
63.3
Non-Hispanic black
27.0
39.4
30.2
30.4
6.2
5.9
7.0
6.2
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
Others
................................................................................................................................................................................................................................................................................................................................................................................
Stage at diagnosis
.......................................................................................................................................................................................................................................................................................................................................................................
CIN 2
64.8
38.5
CIN 3 and in situ
35.2
20.9
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
Local
50.0
11.5
Regional
39.6
9.1
Distant
10.4
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
2.4
.......................................................................................................................................................................................................................................................................................................................................................................
Unstaged
100.0
17.8
................................................................................................................................................................................................................................................................................................................................................................................
Comorbidity index
.......................................................................................................................................................................................................................................................................................................................................................................
85.4
58.8
81.7
78.6
.......................................................................................................................................................................................................................................................................................................................................................................
11.3
22.1
10.5
13.6
3.1
16.4
7.0
6.9
Missing
0.2
2.7
0.9
0.9
Preenrolled
15.8
23.0
15.1
17.3
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................................................................................
Medicaid eligibility groups
.......................................................................................................................................................................................................................................................................................................................................................................
BCCPTA
98.5
55.2
94.2
87.8
Disable
0.2
23.6
2.0
5.9
Others
1.3
21.2
3.8
6.3
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................................................................................
Enrollment status
.......................................................................................................................................................................................................................................................................................................................................................................
Duration, mean (SD)
20.2 (5.1)
17.9 (7.0)
19.8 (5.6)
19.6 (5.7)
Enrolled over 24 mo (Yes)
49.2
41.0
46.5
46.8
.......................................................................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................................................................................
Residence
.......................................................................................................................................................................................................................................................................................................................................................................
Central city large metro
33.9
30.0
35.8
33.4
Fringe county large metro
24.3
40.5
28.5
28.8
Small metropolitan area
35.4
25.7
31.1
32.4
6.2
3.8
4.7
5.4
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
.......................................................................................................................................................................................................................................................................................................................................................................
Completely rural
.......................................................................................................................................................................................................................................................................................................................................................................
Missing
0.2
0.0
0.0
0.1
................................................................................................................................................................................................................................................................................................................................................................................
% households income $15K
26.3 (9.2)
23.7 (9.8)
25.4 (9.2)
25.5 (9.4)
Resident county with a CoC approval hospital
36.1
51.1
41.0
40.4
................................................................................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................................................................................
Ob/Gyn per 1000 women
0.21 (0.18)
0.26 (0.20)
0.24 (0.20)
0.22 (0.19)
................................................................................................................................................................................................................................................................................................................................................................................
BCCPTA, Breast and Cervical Cancer Patient Treatment Act; CoC, Commission on Cancer.
Chien. Cervical cancer treatment under BCCPTA. Am J Obstet Gynecol 2011.
JUNE 2011 American Journal of Obstetrics & Gynecology
533.e3
Research
Oncology
www.AJOG.org
FIGURE 1
Cervical treatment of patients with preinvasive
and invasive cervical cancer under Medicaid
Chien. Cervical cancer treatment under BCCPTA. Am J Obstet Gynecol 2011.
treatment options, we adopted Romanos29 modification of the comorbidity
index originally developed by Charlson.30,31 All available medical claims up
to 1 year after the first month of Medicaid enrollment were used to compute the
Charlson comorbidity index, and patients were assigned the maximal score
observed.
Because reasons for enrollment in Medicaid vary, we hypothesized that women
who enrolled in Medicaid before cancer diagnosis would be a distinct group compared with women who enrolled in Medicaid after their cancer diagnosis. Thus, we
created a dichotomous variable preenrolled to indicate whether subjects were
previously enrolled in Medicaid 4 or more
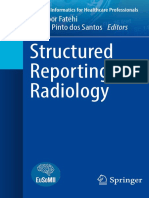
FIGURE 2
The treatment pattern of patients with preinvasive cervical disease
Chien. Cervical cancer treatment under BCCPTA. Am J Obstet Gynecol 2011.
533.e4
American Journal of Obstetrics & Gynecology JUNE 2011
months before the month of their cancer
diagnosis as recorded in the GCCR.
Medicaid eligibility category was defined based on the most frequent eligibility
category during the initial 6 months of enrollment and classified into 3 categories:
(1) BCCPTA, (2) disabled, and (3) other
eligibility groups. We also created a hierarchy to break a tie (eg, BCCPTA before disabled and disabled before the other Medicaid). Finally, length of enrollment was
defined as a dichotomous variable, which
denoted whether she was continuously
enrolled in Medicaid for 24 months or
longer.
County covariates included: (1) urban/rural status of resident county,
(2) percentage of households income
$15K, (3) whether county has at least 1
hospital with CoC certification, and (4)
percentage of Obstetrician/Gynecologist
(Ob/Gyn) per 1000 women.
Statistical analysis
Logistic regressions were used to estimate the odd ratios (ORs) of independent variables associated with the receipt
of cervical cancer treatment. All analyses
were conducted using STATA version
9.2 (STATA Corp, College Station, TX).
R ESULTS
Basic characteristics
The patients (Table 1) with preinvasive
cervical disease (59%) exceed those with
invasive (23%) or unstaged cervical cancer
(18%). A large proportion of patients with
precancerous disease were between the
ages of 19 and 24 (41.7%), non-Hispanic
white (66.8%), with CIN 2 stage (64.8%),
and no comorbidity (85.4%). A full 98.5%
were enrolled under the BCCPTA eligibility category, whereas 15.8% enrolled before their cancer diagnosis (preenrolled)
and 49.2% were enrolled for over 24
months. The mean duration of enrollment
for this group was 20 months in 2-year follow-up period.
Compared with preinvasive cases, we
found that invasive cancer patients were
older, more likely to be non-Hispanic
black, with higher comorbidities, and
more likely to be preenrolled but less
likely to enroll under BCCPTA or be enrolled over 24 months. With respect to
county variations, they were more likely
Oncology
www.AJOG.org
to reside in a county with a higher income population and Ob/Gyn per 1000
women but with no hospital with CoC
approval, relative to their counterparts.
Descriptive analysis
Figure 1 showed the types of cervical
cancer treatment patients received
within 2 years of Medicaid enrollment.
For patients with preinvasive cervical
disease, 56% had any cancer workup,
75% had any precancerous procedure,
and 21% had a simple hysterectomy. For
patients with invasive cervical cancer,
85% had any cancer workup, 34% had
any invasive surgery, 62% had any radiation, and 54% had any chemotherapy.
As further explored, the choices of
treatment among the preinvasive cervical patients, 75% had precancerous procedures, 8% had simple hysterectomy,
and 13% had both treatments. Less than
1% of these patients received only radiation and/or chemotherapy and 4% received no treatment for their disease
(Figure 2). For invasive cases, overall,
15% had invasive surgery, 51% had radiation and/or chemotherapy, 17% had
both, and 18% received no cancer treatment (Figure 3). While we additionally
discussed the treatment according to
stage of cancer, surgery was a major procedure for treating patients with local
stage (29%), whereas radiation and/or
chemotherapy were mainly used for
treating those with regional or distant
(69% and 78%). We also found that patients with local stage of cervical cancer
had the highest rate (24%) of no treatment or minimal treatment (only 32% of
them receiving a conization).
Multivariate analysis
Table 2 showed summary multiple regression results (only significant variables) on the receipt of any cancer
workup, precancerous procedure, and
simple hysterectomy among patients
with preinvasive disease. Patients at an
older age, with a comorbidity, and continuously enrolled over 24 months were
more likely to receive any cancer workup.
Those more likely to receive precancerous procedures were those of younger
age, non-Hispanic black, CIN 2 disease,
with no comorbidity, and residing in a
Research
FIGURE 3
The treatment pattern of patients with invasive cervical cancer
nvasive surgicaal treatment
In
Raadiation and/or chemo
nvasive surgicaal treatment + radiation and
d/or chemo
In
None
24%
100%
15%
199%
7%
699%
78%
2%
%
0%
Distant
17%
30%
29%
Local
Regiional
18%
%
17%
%
50%
%
15%
%
Overall
Chien. Cervical cancer treatment under BCCPTA. Am J Obstet Gynecol 2011.
county with a CoC approval hospital. In
contrast, those more likely to receive surgery (simple hysterectomy) were those of
older age, more advanced stage, and a
comorbidity.
Among invasive cases (Table 3), patients with later stage, higher comorbidity, preenrolled, enrolled under BCCPTA,
and enrolled over 24 months were more
likely to receive any cancer workup.
Non-Hispanic blacks were significantly
less likely to have invasive surgery after
controlling for the other covariates (P
.05). Later stage was associated with
higher odds of radiation or chemotherapy but not surgery. BCCPTA women
were no different in terms of receiving
invasive surgery, radiation, or chemotherapy than other eligibility groups,
whereas patients who were disabled were
less like to undergo surgery compared
with their counterparts.
C OMMENTS
BCCPTA is a policy approach for addressing the challenges of the uninsured
facing serious illness by providing cancer
treatment through a special Medicaid eligibility option. Our study found that
virtually all of the patients with preinva-
sive cervical disease received some form
of treatment. This is extremely important from a policy perspective because
early detection and appropriate treatment of precancerous cells can prevent
them from becoming cancerous and the
treatment is more likely to be successful.
Unfortunately, there were 24% of patients diagnosed with local invasive
cervical cancer who did not receive invasive surgery, radiation, or chemotherapy
based on our analysis of Medicaid claims
data. We did further analysis of these
patients and found there was no difference between treated and not treated
women by county, at least 1 CoC approval hospital nearby, Ob/Gyn:women
ratio, preenrollment, disability or comorbidities. One difference was that patients without treatment were more
likely to reside in low-income areas (P
.048). Further analysis indicated that a
leading reason for the lack of treatment
was disenrollment from Medicaid. Of
those patients who were continuously
enrolled in Medicaid over our 2-year
study period; there was only 6% who did
not have any follow-up treatment. Although even this percentage is concerning, we cannot observe treatment out-
JUNE 2011 American Journal of Obstetrics & Gynecology
533.e5
Research
Oncology
www.AJOG.org
TABLE 2
The summary results of multiple regression analysis for patients
with preinvasive disease under BCCPTA (n 1147)
Dependent variables
Independent variables
Any cancer workup
Age at enrollment, y
OR
95% CI
..........................................................................................................................................................
19-24
0.42 0.240.71
25-34
0.41 0.240.71
35-44
0.38 0.210.68
..........................................................................................................................................................
..........................................................................................................................................................
...................................................................................................................................................................
Comorbidity index
..........................................................................................................................................................
1.81 1.202.72
3.39 1.428.09
..........................................................................................................................................................
...................................................................................................................................................................
Enrolled over 24 mo
1.54 1.201.98
..............................................................................................................................................................................................................................................
Any precancerous procedure Age at enrollment, y
..........................................................................................................................................................
19-24
15.73 8.9127.77
25-34
4.51 2.707.55
..........................................................................................................................................................
...................................................................................................................................................................
Race/ethnicity
..........................................................................................................................................................
Non-Hispanic black
1.92 1.292.86
..........................................................................................................................................................
Others
1.92 1.013.64
...................................................................................................................................................................
CIN 3 and in situ
0.37 0.270.51
...................................................................................................................................................................
Resident county with a CoC approval hospital 1.89 1.143.13
..............................................................................................................................................................................................................................................
Simple hysterectomy
Age at enrollment, y
..........................................................................................................................................................
19-24
0.03 0.020.06
25-34
0.20 0.120.34
..........................................................................................................................................................
...................................................................................................................................................................
Non-Hispanic black
0.48 0.310.76
CIN 3 and in situ
3.87 2.735.48
...................................................................................................................................................................
...................................................................................................................................................................
Comorbidity index
..........................................................................................................................................................
1.62 1.012.60
...................................................................................................................................................................
Resident county with a CoC approval hospital 0.53 0.300.94
..............................................................................................................................................................................................................................................
Covariates included age at enrollment, race/ethnicity, stage of disease, comorbidity, preenrolled, enrolled over 24 mo,
residence county variables (rural/urban, percentage households income $15K, with a CoC approval hospital, percentage
Ob/Gyn per 1000 women).
BCCPTA, Breast and Cervical Cancer Patient Treatment Act; CI, confidence interval; CoC, Commission on Cancer; OR, odds
ratio.
Chien. Cervical cancer treatment under BCCPTA. Am J Obstet Gynecol 2011.
side of Medicaid coverage and these
women may have received cancer treatment either through private insurance, a
clinical trial or even a Medicaid program
in another state. In contrast, we were unable to control for nonclinical factors
affecting treatment, such as patient refusal because of individual beliefs or
preferences.
In our analysis of invasive cases with
none of the treatments identified for invasive cases, 32% of the women received
a conization as part of their evaluation. If
their stage of invasive cancer was stage
1AI, then the conization would have
533.e6
been diagnostic and therapeutic. However, if their disease was more advanced,
then the conization was only diagnostic.
Although the observed treatment may be
appropriate based on this more specific
stage, such information was not available
to us.
Several covariates affect the patterns of
cervical cancer treatment. Younger
women were less likely to undergo surgery because of childbearing age.32 Similar to previous work,33,34 we found that
non-Hispanic black patients were less
likely to receive surgical treatment for
both preinvasive and invasive cervical
American Journal of Obstetrics & Gynecology JUNE 2011
cases. The potential impact of BCCPTA
on the care of these patients is needed as
the lower hysterectomy rate may be associated with higher mortality if this is
the necessary treatment for the stage of
disease found among these minority
populations.
Another previous study indicated that
the average cost of BCCPTA women
with cervical cancer was lower than those
under the disabled category, whereas
higher than those under other Medicaid
categories.23 Our results might reflect
that the Georgia BCCPTA program used
the Medicaid funding effectively to treat
more women with cervical cancer and at
a relatively lower cost.
It is important to note that preinvasive
cervical patients who lived in a county
that has at least 1 CoC approval hospital
were likely to receive nonsurgical treatment and were less likely to have a hysterectomy. This might reflect that CoC
approval hospitals are more likely to
consider possible alternative treatment
options because they have more specialists and training in oncology.
The advantage of this study is that we
were able to identify cancer treatment
through Medicaid claims beyond the period covered by the GCCR, which captures information about incident cancers and the use of initial surgery or
radiation. Medicaid data allow for tracking patients longitudinally for receipt of
chemotherapy or drugs and information
other than vital status. Linked registry
and Medicaid data have the potential to
identify appropriate, timely cancer treatment and can thereby serve to gauge
quality of care among these low-income
patients. This is important because the
intervening years before health reform
can be used to further address the unnecessary morbidity and mortality associated with cervical cancer.
Lack of insurance coverage is traditionally seen as the main reason for
patients not getting timely and appropriate treatment. However, this study found
that getting insurance through BCCPTA
is only part of the solution to help previously uninsured low-income women diagnosed with those cancers to get treatment. This was found in another study
that used SEER data and showed that
Oncology
www.AJOG.org
nearly 11% of the lowest-income patients diagnosed with invasive cervical
cancer received no treatment. To increase the rate of treatment in this vulnerable group, patient navigation intervention might have an impact. It has been
shown to successfully improve mammography screening rates for low-income minority populations in several studies.37-40
Relevant to our study population, a patient
navigation system for women with breast
cancer and a Community Health Advocates (CHA) program implemented
through Atlantas inner-city hospital led to
an increase in stage 0 breast cancer cases
from 12.4% to 25.8%; the vast majority of
participating women were African-American.41 Clearly devoting financial resources
to patient navigation for cervical cancer as
with breast cancer may improve patient
follow-up in this vulnerable group.
Although this is one of the few studies
to examine BCCPTA women, there are
several limitations. First, the data cannot
be generalized as states operate BCCPTA
programs differently. Moreover, Georgia is 1 of 12 states that selected the most
expansive coverage,35 which potentially
enrolled more uninsured women. This
greater access might result in larger variation in cervical cancer treatment patterns compared with states with more restrictive coverage.
Second, although the optimal treatment
is largely based on stage of disease, the
womans age and her childbearing plans,
and physicians and patients preferences
are part of the decision process36 and we
were not able to control for unseen variation (eg, individual preferences) that likely
affect treatment decisions.
We were unable to track patients cervical cancer treatment if their treatment was
out of Medicaid claims, out of the study
period, or out of cancer treatment as we
defined it. In addition, we would not know
the treatment patterns of those who enrolled in Medicaid more than 6 months after diagnosis. Those patients might have
enrolled in Medicaid under BCCPTA but
actually received treatment before enrolling. Finally, we found that 4% of preinvasive cervical cases received chemotherapy
that might not be clinically appropriate;
these women may have other types of cancer that we were unable to detect.
Research
TABLE 3
The summary results of multiple regression analysis for patients
with invasive cervical cancer under BCCPTA (n 444)
Dependent variables
Independent variables
Any cancer workup
Stage of disease
OR
95% CI
...................................................................................................................................................
Regional
3.03
1.545.98
Distant
6.55
1.6526.05
...................................................................................................................................................
............................................................................................................................................................
Comorbidity index
...................................................................................................................................................
3.27
1.387.75
...................................................................................................................................................
5.68
1.7618.28
Preenrolled
2.85
1.316.23
BCCPTA
4.09
1.878.94
Enrolled over 24 mo
2.40
1.214.76
Non-Hispanic black
0.61
0.371.00
............................................................................................................................................................
............................................................................................................................................................
............................................................................................................................................................
..............................................................................................................................................................................................................................................
Any invasive surgery
............................................................................................................................................................
Stage of disease
...................................................................................................................................................
Regional
0.32
0.200.52
Distant
0.10
0.030.32
Preenrolled
2.08
1.133.85
Disabled
0.29
0.140.64
...................................................................................................................................................
............................................................................................................................................................
............................................................................................................................................................
..............................................................................................................................................................................................................................................
Any radiation
Stage of disease
...................................................................................................................................................
Regional
10.25
5.8218.06
Distant
6.36
2.7014.95
...................................................................................................................................................
............................................................................................................................................................
Comorbidity index
...................................................................................................................................................
2.39
1.154.99
2.01
1.193.39
............................................................................................................................................................
Enrolled over 24 mo
..............................................................................................................................................................................................................................................
Any chemotherapy
Stage of disease
...................................................................................................................................................
Regional
5.57
3.439.03
Distant
3.98
1.908.32
...................................................................................................................................................
............................................................................................................................................................
Comorbidity index
...................................................................................................................................................
2.22
1.184.20
..............................................................................................................................................................................................................................................
Covariates included age at enrollment, race/ethnicity, stage of disease, comorbidity, preenrolled, Medicaid eligibility groups,
enrolled over 24 mo, residence county variables (rural/urban, percentage households income $15K, with a CoC approval
hospital, percentage Ob/Gyn per 1000 women).
BCCPTA, Breast and Cervical Cancer Patient Treatment Act; CI, confidence interval; CoC, Commission on Cancer; OR, odds
ratio.
Chien. Cervical cancer treatment under BCCPTA. Am J Obstet Gynecol 2011.
In summary, cervical cancer is highly
preventable and curable when it is detected
early and treated effectively. The creation
of the BCCPTA provides a pathway for
those uninsured women diagnosed with
preinvasive and invasive cervical disease
into Medicaid and treatment. Our data
showed that the Georgia Medicaid might
improve the health of previously uninsured women diagnosed with this disease.
Extension of treatment to patients with
preinvasive conditions is a highly effective
use of public program funds because it
can prevent the disease from becoming
invasive.
f
ACKNOWLEDGEMENT
We thank Dr Victor Wu for his assistance in
classifying procedure and CPT codes into different treatment groups.
REFERENCES
1. What are the key statistics about cervical
cancer? 2009. Available at: http://www.cancer.
JUNE 2011 American Journal of Obstetrics & Gynecology
533.e7
Research
Oncology
org/docroot/CRI/content/CRI_2_4_1X_What_
are_the_key_statistics_for_cervical_cancer_8.
asp?rnavcri. Accessed July 21, 2009.
2. Schoell WMJ, Janicek MF, Mirhashemi R.
Epidemiology and biology of cervical cancer.
Sem Surg Oncol 1999;16:203-11.
3. Devesa SS, Silverman DT, Young JLJ, et al.
Cancer incidence and mortality trends among
whites in the United States, 1947-84. J Natl
Cancer Inst 1987;79:701-70.
4. Casper MJ, Clarke AE. Making the Pap
smear into the Right Tool for the job, cervical
cancer screening in the USA, circa 1940-95.
Soc Stud Sci 1998;28:255-90.
5. Bradley CJ, Given CW, Roberts C. Health
care disparities and cervical cancer. Am J Public Health 2004;94:2098-103.
6. Akers AY, Newmann SJ, Smith JS. Factors
underlying disparities in cervical cancer incidence, screening, and treatment in the United
States. Curr Prob Cancer 2007;31:157-81.
7. Breen N, Wagener DK, Brown ML, Davis
WW, Ballard-Barbash R. Progress in cancer
screening over a decade: results of cancer
screening from the 1987, 1992, and 1998 National Health Interview Surveys. J Natl Cancer
Inst 2001;93:1704-13.
8. Sung JFC, Alema-Mensah E, Blumenthal DS.
Inner-city African American women who failed to
receive cancer screening following a culturallyappropriate intervention: the role of health insurance. Cancer Detect Prevent 2002;26:28-32.
9. Hewitt M, Devesa SS, Breen N. Cervical cancer screening among U.S. women: analyses of
the 2000 National Health Interview Survey. Prevent Med 2004;39:270-8.
10. Roetzheim RG, Pal N, Tennant C, et al. Effects of health insurance and race on early
detection of cancer. J Natl Cancer Inst 1999;
91:1409-15.
11. Rodriguez MA, Ward LM, Perez-Stable EJ.
Breast and cervical cancer screening: impact of
health insurance status, ethnicity, and nativity of
Latinas. Ann Fam Med 2005;3:235-41.
12. Harlan LC, Greene AL, Clegg LX, Mooney M,
Stevens JL, Brown ML. Insurance Status and the
use of guideline therapy in the treatment of selected cancers. J Clin Oncol 2005;23:9079-88.
13. Thorpe KE, Howard D. Health insurance
and spending among cancer patients. Health
533.e8
www.AJOG.org
Aff (Millwood). 2003 Jan-Jun;Suppl Web
Exclusives:W3-189-98.
14. Miller B, Ries L, Hankey B, Kosary C. SEER
Cancer Statistics Review: 1973-1990. Betheseda: National Cancer Institute; 1993.
15. Weiss L, Kau T, Sparks B, Swanson G.
Trends in cervical cancer incidence among
young black and white women in metropolitan
Detroit. Cancer 1994;73:1849-54.
16. Mangan SA, Legano LA, Rosen CM, et al.
Increased prevalence of abnormal Papanicolaou smears in urban adolescents. Arch Pediatr
Adolesc Med 1997;151:481-4.
17. Center for Disease Control and Prevention.
National breast and cervical cancer early detection program. Atlanta, GA: CDC; 2009.
18. About the program. 2009. Available at:
http://www.cdc.gov/cancer/NBCCEDP/about.
htm. Accessed July 21, 2009,
19. Adams EK, Florence CS, Thorpe KE, Becker
ER, Joski PJ. Preventive care: female cancer
screening, 1996-2000. Am J Prevent Med
2003;25:301-7.
20. Chattopadhyay SK, Hall HI, Wolf RB, Custer
WS. Sources of health insurance in the U.S.:
analysis of state-level data and implications for
public health programs. J Public Health Manage Pract 1999;5:35-46.
21. Paula ML, Lisa CR, Debra JM, Lisa RS,
Donna BK, Lowell ES. Strategies for follow-up
and treatment services in state breast and cervical cancer screening programs. Womens
Health Issues 1999;9:42-9.
22. Medicaid Eligibility Overview. CMS, 2009. Available at: http://www.cms.hhs.gov/Medicaid
Eligibility/01_Overview.asp. Accessed Feb. 20,
2009.
23. Adams EK, Blake SC, Raskind-Hood C, et
al. The Breast and Cervical Cancer Prevention
and Treatment Act (BCCPTA) in Georgia:
women covered and Medicaid costs in 2003. J
Georgia Public Health Assn 2007;1:1-10.
24. Adams EK, Chien L-N, Florence CS, Raskind-Hood C. The Breast and Cervical Cancer
Prevention and Treatment Act in Georgia.
Cancer 2009;115:1300-9.
25. Chien L-N, Adams EK. The effect of the
Breast and Cervical Cancer Prevention and
Treatment Act on Medicaid disenrollment.
Womens Health Issues 2010;20:266-71.
American Journal of Obstetrics & Gynecology JUNE 2011
26. About the CoC. 2008. Available at: http://
www.facs.org/cancer/coc/cocar.html#appr. Accessed Dec. 5, 2008.
27. Complete census 2000 data and boundary
files in easy-to-use CD-ROM formatFirst
Public Demonstration at International Council of
Shopping Centers Conference. Available at:
http://www.caci.com/about/news/05_21_01_
2_NR.html. Accessed June 2, 2010.
28. Cervical Cancer Treatment (PDQ): Health
Professional Version, 2010. Available at: http://
www.cancer.gov/cancertopics/pdq/treatment/
cervical/healthprofessional. Accessed June 2,
2010.
29. Romano PS, Roost LL, Jollis JG. Presentation adapting a clinical comorbidity index for use
with ICD-9-CM administrative data: differing perspectives. J Clin Epidemiol 1993;46:1075-9.
30. Klabunde CN, Potosky AL, Legler JM, Warren JL. Development of a comorbidity index using physician claims data. J Clin Epidemiol
2000;53:1258-67.
31. Klabunde CN, Warren JL, Legler JM. Assessing comorbidity using claims data: an overview. Med Care 2002;40:IV-26-35.
32. van der Aa MA, Siesling S, Poll-Franse
LVvd, Schutter EM, Lybeert ML, Coebergh
JWW. Age-specific differences in the treatment of cervical cancer in the east and the
south of The Netherlands 1989-2004. Eur J
Obstet Gynecol Reprod Biol 2009;147:
78-82.
33. del Carmen MG, Montz FJ, Bristow RE, Bovicelli A, Cornelison T, Trimble E. Ethnic differences in patterns of care of stage 1A1 and
stage 1A2 cervical cancer: a SEER database
study. Gynecol Oncol 1999;75:113-7.
34. Shavers VL, Brown ML. Racial and ethnic
disparities in the receipt of cancer treatment.
J Natl Cancer Inst 2002;94:334-57.
35. Breast and cervical cancer prevention and
treatment activity map. Available at: http://
www.cms.hhs.gov/MedicaidSpecialCovCond/
Downloads/BREASTandCERVICALCANCER
PREVENTIONandTREATMENTACTIVITYMAP.pdf.
Accessed Jan. 12, 2010.
36. Cervical Cancer Treatment (PDQ): Health
Professional Version, 2010. Available at: http://
www.cancer.gov/cancertopics/pdq/treatment/
cervical/healthprofessional. Accessed June 2,
2010.
S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Digital Mammography: Mammograph FFDM - Mammograph D-TomoDocument21 paginiDigital Mammography: Mammograph FFDM - Mammograph D-TomoBrahim lahmaidÎncă nu există evaluări
- Euref Tomo Protocol Version 015Document71 paginiEuref Tomo Protocol Version 015fysmaÎncă nu există evaluări
- Breast - DCIS.Bx 1.0.1.0.REL CAPCPDocument6 paginiBreast - DCIS.Bx 1.0.1.0.REL CAPCPkarimahihdaÎncă nu există evaluări
- Breast UltrasoundDocument35 paginiBreast Ultrasoundseb2008Încă nu există evaluări
- Denial - Primary Reason Code DescriptionsDocument21 paginiDenial - Primary Reason Code Descriptionsfahhad lashari100% (1)
- Breast Imaging The Requisites 3Rd Edition Debra M Ikeda Full ChapterDocument67 paginiBreast Imaging The Requisites 3Rd Edition Debra M Ikeda Full Chapterrosa.jenkins735100% (5)
- Interventional Ultrasound in Obstetrics, Gynaecology and The BreastDocument286 paginiInterventional Ultrasound in Obstetrics, Gynaecology and The BreastDiana-Elena Comandasu100% (2)
- 2021 Batangas Medical Center - Updated Citizens Charter HandbookDocument447 pagini2021 Batangas Medical Center - Updated Citizens Charter HandbookHarlyn MagsinoÎncă nu există evaluări
- Dimitar Petrov PhDthesisDocument166 paginiDimitar Petrov PhDthesismartuflashÎncă nu există evaluări
- Breast and Cervical Cancer Screening in The Philippines Challenges and Steps ForwardDocument3 paginiBreast and Cervical Cancer Screening in The Philippines Challenges and Steps ForwardAlyssa MarzanÎncă nu există evaluări
- Breast Schwartz 2015 10th EditionDocument141 paginiBreast Schwartz 2015 10th EditionKlaire LodroñoÎncă nu există evaluări
- Mammography Sas 10Document11 paginiMammography Sas 10faith mari madrilejosÎncă nu există evaluări
- BreastDocument50 paginiBreastعلي عليÎncă nu există evaluări
- QR Management of Breast Cancer (3rd Ed)Document8 paginiQR Management of Breast Cancer (3rd Ed)Jye yiÎncă nu există evaluări
- The M.D. Anderson Surgical Oncology Handbook-2011 PDFDocument920 paginiThe M.D. Anderson Surgical Oncology Handbook-2011 PDFjimdioÎncă nu există evaluări
- Benign Vs Malignant Masses in Breast UltrasoundDocument95 paginiBenign Vs Malignant Masses in Breast UltrasoundWidya Surya AvantiÎncă nu există evaluări
- How To Assess Breast DraftDocument5 paginiHow To Assess Breast DraftLuckyÎncă nu există evaluări
- (4X - A5) - 08161373182 - Shelf-Life Obgyn 2015 PDFDocument358 pagini(4X - A5) - 08161373182 - Shelf-Life Obgyn 2015 PDFcmbhganteng80% (5)
- Combined Orals APGODocument52 paginiCombined Orals APGOEmilee Tu0% (1)
- Evwoman M00o03Document33 paginiEvwoman M00o03Nader AlsheikhÎncă nu există evaluări
- 2022 Book StructuredReportingInRadiologyDocument189 pagini2022 Book StructuredReportingInRadiologyHipatia SanchezÎncă nu există evaluări
- Fi Bro AdenomaDocument2 paginiFi Bro AdenomafebrianaayupÎncă nu există evaluări
- Public Health - Resume of Shah BookDocument54 paginiPublic Health - Resume of Shah BookKami Dhillon83% (6)
- Mammography PresentationDocument84 paginiMammography Presentationsarose bhandari67% (3)
- Medical Facts and MCQ'S - Breast MCQDocument22 paginiMedical Facts and MCQ'S - Breast MCQTony Dawa0% (1)
- Hologic Selenia Tech WorkbookDocument53 paginiHologic Selenia Tech WorkbookEric F. Davis80% (5)
- Vilas County News-Review, Oct. 5, 2011 - SECTION CDocument14 paginiVilas County News-Review, Oct. 5, 2011 - SECTION CNews-ReviewÎncă nu există evaluări
- A New Approach To Breast Cancer Terminology Based On The A - 2022 - European JouDocument21 paginiA New Approach To Breast Cancer Terminology Based On The A - 2022 - European JouWang YuÎncă nu există evaluări
- DR Tech Company PresentationDocument38 paginiDR Tech Company PresentationPopescu ValiÎncă nu există evaluări
- Breast Cancer: Prima Medika HospitalDocument35 paginiBreast Cancer: Prima Medika HospitalPrima MedikaÎncă nu există evaluări