S-ar putea să vă placă și
- Auriculo Research PDFDocument18 paginiAuriculo Research PDFOdin Tachón100% (1)
- Acupuncture 3-Points For AutismDocument3 paginiAcupuncture 3-Points For AutismHaryono zhu100% (1)
- Isaac Asimov - "Nightfall"Document20 paginiIsaac Asimov - "Nightfall"Aditya Sharma100% (1)
- The Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1De la EverandThe Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1Evaluare: 5 din 5 stele5/5 (1)
- EMC Design Guide For PCBDocument78 paginiEMC Design Guide For PCBFaruq AhmedÎncă nu există evaluări
- Clinical Application Meridian Diagnosis-FratkinDocument20 paginiClinical Application Meridian Diagnosis-Fratkinocoxodo100% (3)
- Acupuncture Bell's Palsy RecoveryDocument7 paginiAcupuncture Bell's Palsy RecoveryJk SalvadorÎncă nu există evaluări
- Acupuncture For Cancer PatientsDocument53 paginiAcupuncture For Cancer PatientsElsaCarreira100% (2)
- Creature Loot PDF - GM BinderDocument97 paginiCreature Loot PDF - GM BinderAlec0% (1)
- Auriculo ResearchDocument12 paginiAuriculo Researchtvmedicine100% (1)
- Insomnia 6Document14 paginiInsomnia 6Utomo FemtomÎncă nu există evaluări
- Pelvic PainDocument15 paginiPelvic PainocoxodoÎncă nu există evaluări
- Organic Evolution (Evolutionary Biology) Revised Updated Ed by Veer Bala RastogiDocument1.212 paginiOrganic Evolution (Evolutionary Biology) Revised Updated Ed by Veer Bala RastogiTATHAGATA OJHA83% (6)
- Keb Combivis 6 enDocument232 paginiKeb Combivis 6 enhaithamÎncă nu există evaluări
- Acupuncture Evidence Project - Mcdonald and Janz - Revised Edition 07.02.17 ReferencedDocument81 paginiAcupuncture Evidence Project - Mcdonald and Janz - Revised Edition 07.02.17 ReferencednaturamedicaÎncă nu există evaluări
- YNSADocument8 paginiYNSAGracielle VasconcelosÎncă nu există evaluări
- Acupuncture For AsthmaDocument16 paginiAcupuncture For AsthmaRichard SiahaanÎncă nu există evaluări
- V Ships Appln FormDocument6 paginiV Ships Appln Formkaushikbasu2010Încă nu există evaluări
- AkupunturDocument29 paginiAkupunturNoraÎncă nu există evaluări
- The Recent History of AcupunctureDocument2 paginiThe Recent History of AcupunctureBhaskaranÎncă nu există evaluări
- Homeroom Guidance Grade 12 Quarter - Module 4 Decisive PersonDocument4 paginiHomeroom Guidance Grade 12 Quarter - Module 4 Decisive PersonMhiaBuenafe86% (36)
- Acupressure: The Evidence Presses On: Publication Info: Alternative Medicine Alert Atlanta (Jun 2012)Document5 paginiAcupressure: The Evidence Presses On: Publication Info: Alternative Medicine Alert Atlanta (Jun 2012)NoeRhul M-lhati OelfhaÎncă nu există evaluări
- Acupuncture - 11 10 2015Document6 paginiAcupuncture - 11 10 2015Rafael EscalanteÎncă nu există evaluări
- Chronic PainDocument13 paginiChronic PainocoxodoÎncă nu există evaluări
- Gynaecology and Acupuncture: Briefing Paper No 4Document9 paginiGynaecology and Acupuncture: Briefing Paper No 4Liliac41Încă nu există evaluări
- Effectiveness Low Back PainDocument14 paginiEffectiveness Low Back PainDianu GutiérrezÎncă nu există evaluări
- Acupuncture Relieves Asthma AttacksDocument4 paginiAcupuncture Relieves Asthma AttacksriezzzadityaÎncă nu există evaluări
- Acupuncture Trial Northern HospitalDocument8 paginiAcupuncture Trial Northern HospitalvicarofskepticÎncă nu există evaluări
- Nursing and Reflexology ResearchDocument39 paginiNursing and Reflexology ResearchJacqueline FerdinandÎncă nu există evaluări
- Children: Acupuncture For Pediatric PainDocument15 paginiChildren: Acupuncture For Pediatric PainRachel GreeneÎncă nu există evaluări
- Menopause Acupuncture: Briefing Paper No 5Document5 paginiMenopause Acupuncture: Briefing Paper No 5Claudia CattaniÎncă nu există evaluări
- Acupuncture and CD4+Document21 paginiAcupuncture and CD4+Hafiz NophafizÎncă nu există evaluări
- Acupuncture Evidence Project TheDocument83 paginiAcupuncture Evidence Project TheAndresFavaPinoÎncă nu există evaluări
- Acupuncture: A Therapeutic Modality, But Not A Placebo: Martin WangDocument74 paginiAcupuncture: A Therapeutic Modality, But Not A Placebo: Martin WangirmaÎncă nu există evaluări
- Meniere's Disease - Case StudyDocument3 paginiMeniere's Disease - Case StudyZORANASNÎncă nu există evaluări
- Acupuncture (Reseach IonDocument17 paginiAcupuncture (Reseach IonRalph NicolasÎncă nu există evaluări
- Patients Experience of AcupunctureDocument7 paginiPatients Experience of AcupunctureJoão PauloÎncă nu există evaluări
- Acupunct Med 2014 p242Document9 paginiAcupunct Med 2014 p242Anonymous PFNzHoÎncă nu există evaluări
- Vs Research Summary 092710Document26 paginiVs Research Summary 092710tomasÎncă nu există evaluări
- Aspirin in Episodic Tension-Type Headache: Placebo-Controlled Dose-Ranging Comparison With ParacetamolDocument9 paginiAspirin in Episodic Tension-Type Headache: Placebo-Controlled Dose-Ranging Comparison With ParacetamolErwin Aritama IsmailÎncă nu există evaluări
- Reduced Health Resource Use After Acupuncture For Low-Back PainDocument2 paginiReduced Health Resource Use After Acupuncture For Low-Back PainTeddy TrickserÎncă nu există evaluări
- Acupressure Evidence and Research Opportunities for Symptom ManagementDocument21 paginiAcupressure Evidence and Research Opportunities for Symptom ManagementalwiyaÎncă nu există evaluări
- Is Most of Acupuncture Research A Sham 2009Document4 paginiIs Most of Acupuncture Research A Sham 2009Victor Manuel Enriquez GÎncă nu există evaluări
- Acupuncture Is Underutilized in Hospice and Palliative MedicineDocument11 paginiAcupuncture Is Underutilized in Hospice and Palliative MedicinetvmedicineÎncă nu există evaluări
- Review ArticleDocument15 paginiReview ArticleAugustinÎncă nu există evaluări
- Arthritis & Rheumatism: Acupuncture For Treating Osteoarthritis of The Knee and The HipDocument3 paginiArthritis & Rheumatism: Acupuncture For Treating Osteoarthritis of The Knee and The Hipunbelievable686Încă nu există evaluări
- Ejp 26 1006Document15 paginiEjp 26 1006Sam SamÎncă nu există evaluări
- Placebo FinalDocument9 paginiPlacebo FinalRica Jane TorresÎncă nu există evaluări
- 233 Full PDFDocument5 pagini233 Full PDFrizk86Încă nu există evaluări
- The Effect of Traditional Chinese Medical Acupuncture (TCM) On Test Anxiety (A Pilot Study)Document8 paginiThe Effect of Traditional Chinese Medical Acupuncture (TCM) On Test Anxiety (A Pilot Study)Chandra MosesÎncă nu există evaluări
- The Efficacy of Acupuncture For The Treatment of Sciatica - A Systematic Review and Meta-AnalysisDocument13 paginiThe Efficacy of Acupuncture For The Treatment of Sciatica - A Systematic Review and Meta-AnalysisDan CarcamoÎncă nu există evaluări
- Acupuncture Against Depression Acupuncture Against Depression Acupuncture Against Depression Acupuncture Against DepressionDocument20 paginiAcupuncture Against Depression Acupuncture Against Depression Acupuncture Against Depression Acupuncture Against DepressionFrancois du RizÎncă nu există evaluări
- Complementary and Alternative Medicine For Functional Gastrointestinal DisordersDocument5 paginiComplementary and Alternative Medicine For Functional Gastrointestinal DisordersRegine Dela peñaÎncă nu există evaluări
- Auriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument12 paginiAuriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsSol Instituto TerapêuticoÎncă nu există evaluări
- Acupuncture For Tension-Type Headache - CochraneDocument4 paginiAcupuncture For Tension-Type Headache - CochraneDaniel Alejandro Vargas PérezÎncă nu există evaluări
- Acupuncture in Patients With Osteoarthritis of The Knee: A Randomised TrialDocument9 paginiAcupuncture in Patients With Osteoarthritis of The Knee: A Randomised TrialDiana PiresÎncă nu există evaluări
- Acupuncture in The Treatment ofDocument9 paginiAcupuncture in The Treatment ofIntan AnanthaÎncă nu există evaluări
- Clinical Hypnosis For The Alleviation of Tinnitus: Thomas E. CopeDocument4 paginiClinical Hypnosis For The Alleviation of Tinnitus: Thomas E. CopeIsabelÎncă nu există evaluări
- Clinical Hypnosis For The Alleviation of TinnitusDocument4 paginiClinical Hypnosis For The Alleviation of TinnitusIsabelÎncă nu există evaluări
- 1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileDocument6 pagini1156 The Effects of Acupuncture Versus Sham Acupuncture in The Treatment of Fibromyalgia A Randomized Controlled Clinical Trial FileValdemar Caumo JuniorÎncă nu există evaluări
- Revisão Crítica Da Acupuntura MédicaDocument9 paginiRevisão Crítica Da Acupuntura MédicaniklukÎncă nu există evaluări
- ECT in Schizophrenia Need For ReappraisalDocument3 paginiECT in Schizophrenia Need For ReappraisalanettewillÎncă nu există evaluări
- Hipnosis Estudio Piloto Holanda 1988Document6 paginiHipnosis Estudio Piloto Holanda 1988Gracia DelgadoÎncă nu există evaluări
- Electroconvulsive TherapyDocument10 paginiElectroconvulsive TherapyYasinÎncă nu există evaluări
- Numero Agh IDocument7 paginiNumero Agh Ialvaedison00Încă nu există evaluări
- Gouty Arthritis PDFDocument8 paginiGouty Arthritis PDFEvan SmixÎncă nu există evaluări
- Acupuncture For Primary Fibromyalgia: Study Protocol of A Randomized Controlled TrialDocument9 paginiAcupuncture For Primary Fibromyalgia: Study Protocol of A Randomized Controlled TrialSILVIA ROSARIO CHALCO MENDOZAÎncă nu există evaluări
- Acupuncture Musculoskeletal ReviewDocument82 paginiAcupuncture Musculoskeletal ReviewSaurav GuptaÎncă nu există evaluări
- HerbclipDocument2 paginiHerbclipocoxodoÎncă nu există evaluări
- CoverDocument15 paginiCoverocoxodoÎncă nu există evaluări
- A Guide To Reading - 9781606209738Document45 paginiA Guide To Reading - 9781606209738Scarlet PimpernelÎncă nu există evaluări
- HerbsDocument6 paginiHerbsocoxodoÎncă nu există evaluări
- Chapt 01Document12 paginiChapt 01ocoxodoÎncă nu există evaluări
- MeetingDocument4 paginiMeetingocoxodoÎncă nu există evaluări
- First Family TasajaraDocument278 paginiFirst Family TasajaraocoxodoÎncă nu există evaluări
- Guasha PainDocument5 paginiGuasha PainocoxodoÎncă nu există evaluări
- Treating Musculo-Skeletal Pain With Traditional Chinese MedicineDocument2 paginiTreating Musculo-Skeletal Pain With Traditional Chinese MedicineocoxodoÎncă nu există evaluări
- A Grammar of The Arabic LanguageDocument378 paginiA Grammar of The Arabic LanguagemanelaoÎncă nu există evaluări
- Pain BadDocument4 paginiPain BadocoxodoÎncă nu există evaluări
- Neck PainDocument6 paginiNeck PainocoxodoÎncă nu există evaluări
- PainDocument6 paginiPainocoxodoÎncă nu există evaluări
- Neck PainDocument2 paginiNeck PainocoxodoÎncă nu există evaluări
- Chronic PainDocument6 paginiChronic PainocoxodoÎncă nu există evaluări
- Analgesic Mechanism of Electroacupuncture in An Arthritic Pain Model of Rats: A Neurotransmitter StudyDocument6 paginiAnalgesic Mechanism of Electroacupuncture in An Arthritic Pain Model of Rats: A Neurotransmitter Studyocoxodo0% (1)
- Hypothesis: Placebo Analgesia, Acupuncture and Sham SurgeryDocument6 paginiHypothesis: Placebo Analgesia, Acupuncture and Sham SurgeryHeHICÎncă nu există evaluări
- PainDocument6 paginiPainocoxodoÎncă nu există evaluări
- Research Article: Effects of Electroacupuncture at BL60 On Formalin-Induced Pain in RatsDocument7 paginiResearch Article: Effects of Electroacupuncture at BL60 On Formalin-Induced Pain in RatsocoxodoÎncă nu există evaluări
- PainDocument9 paginiPainocoxodoÎncă nu există evaluări
- Measures A: J. B. P. StephensonDocument2 paginiMeasures A: J. B. P. StephensonocoxodoÎncă nu există evaluări
- PainDocument26 paginiPainocoxodoÎncă nu există evaluări
- PainDocument9 paginiPainocoxodoÎncă nu există evaluări
- Post AnestesiaDocument7 paginiPost AnestesiaocoxodoÎncă nu există evaluări
- AnestesiaDocument4 paginiAnestesiaocoxodoÎncă nu există evaluări
- PainDocument7 paginiPainocoxodoÎncă nu există evaluări
- Pain BJMDocument15 paginiPain BJMocoxodoÎncă nu există evaluări
- Canary TreatmentDocument117 paginiCanary TreatmentRam KLÎncă nu există evaluări
- What Is Gross Income - Definition, Formula, Calculation, and ExampleDocument7 paginiWhat Is Gross Income - Definition, Formula, Calculation, and ExampleKapil SharmaÎncă nu există evaluări
- Pneapple Waste To Bioethanol Casabar - Et - Al-2019-Biomass - Conversion - and - BiorefineryDocument6 paginiPneapple Waste To Bioethanol Casabar - Et - Al-2019-Biomass - Conversion - and - Biorefineryflorian willfortÎncă nu există evaluări
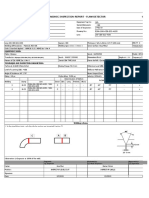
- Ut ProcedureDocument2 paginiUt ProcedureJJ WeldingÎncă nu există evaluări
- Making An Appointment PaperDocument12 paginiMaking An Appointment PaperNabila PramestiÎncă nu există evaluări
- Procedure For NC and CapaDocument2 paginiProcedure For NC and CapaSAKTHIVEL AÎncă nu există evaluări
- PENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIDocument15 paginiPENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIRizky Hizrah WumuÎncă nu există evaluări
- MinistopDocument23 paginiMinistopAlisa Gabriela Sioco OrdasÎncă nu există evaluări
- Reg OPSDocument26 paginiReg OPSAlexandru RusuÎncă nu există evaluări
- Neuroimaging - Methods PDFDocument372 paginiNeuroimaging - Methods PDFliliana lilianaÎncă nu există evaluări
- Counter Circuit Types, Components and ApplicationsDocument22 paginiCounter Circuit Types, Components and Applicationsnavin_barnwalÎncă nu există evaluări
- Data Structures LightHall ClassDocument43 paginiData Structures LightHall ClassIwuchukwu ChiomaÎncă nu există evaluări
- I. Specifikacija Opreme Sa Ugradnjom R.Br. Opis JM KomDocument4 paginiI. Specifikacija Opreme Sa Ugradnjom R.Br. Opis JM KomAleksandar VidakovicÎncă nu există evaluări
- Barker-Choucalas, Vida PDFDocument176 paginiBarker-Choucalas, Vida PDFAnn GarbinÎncă nu există evaluări
- Ajwin Handbuch enDocument84 paginiAjwin Handbuch enEnzo AguilarÎncă nu există evaluări
- Awwa c207 Flanges Spec SheetDocument13 paginiAwwa c207 Flanges Spec SheetVincent DiepÎncă nu există evaluări
- UM Routing L3P 15 01 UsDocument102 paginiUM Routing L3P 15 01 UsmiroÎncă nu există evaluări
- Documentation Control HandbookDocument9 paginiDocumentation Control Handbookcrainvictor 45Încă nu există evaluări
- Chapter 5Document11 paginiChapter 5XDXDXDÎncă nu există evaluări
- Linear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisDocument11 paginiLinear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisPhD EEÎncă nu există evaluări
- Gulfco 1049 MaxDocument5 paginiGulfco 1049 MaxOm Prakash RajÎncă nu există evaluări
- Gr.10 Music History ModuleDocument45 paginiGr.10 Music History ModuleKyle du PreezÎncă nu există evaluări
- Going to the cinema listening practiceDocument2 paginiGoing to the cinema listening practiceMichael DÍligo Libre100% (1)