S-ar putea să vă placă și
- Indications and Usage: M M M M M M M M M M MDocument4 paginiIndications and Usage: M M M M M M M M M M MJesthony Lee CorderoÎncă nu există evaluări
- Amitriptyline PDFDocument3 paginiAmitriptyline PDFscribdseewalÎncă nu există evaluări
- Dextroamphetamine SulfateDocument3 paginiDextroamphetamine Sulfateapi-3797941100% (1)
- The Format of This Leaflet Was Determined by The Ministry of Health and Its Content Was Checked and Approved by It On February 2016Document10 paginiThe Format of This Leaflet Was Determined by The Ministry of Health and Its Content Was Checked and Approved by It On February 2016ddandan_2Încă nu există evaluări
- Droperidol (Inapsine)Document1 paginăDroperidol (Inapsine)EÎncă nu există evaluări
- HaemaccelinfDocument9 paginiHaemaccelinfSisca YulistianaÎncă nu există evaluări
- Drug Study On EPINEPHRINEDocument6 paginiDrug Study On EPINEPHRINEshadow gonzalezÎncă nu există evaluări
- EzetimibeDocument3 paginiEzetimibeapi-3797941Încă nu există evaluări
- Briviact Film-Coated Tablets Summary of Product CharacteristicsDocument110 paginiBriviact Film-Coated Tablets Summary of Product CharacteristicsBendisDacicaÎncă nu există evaluări
- Zolpidem TartrateDocument2 paginiZolpidem Tartrateapi-3797941Încă nu există evaluări
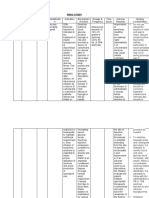
- Generic Classification Dosage Mechanism of Action Indications Adverse ReactionDocument1 paginăGeneric Classification Dosage Mechanism of Action Indications Adverse ReactionKamille Anne Valdez DavidÎncă nu există evaluări
- Side Effects:: AtropineDocument7 paginiSide Effects:: AtropinekletadaÎncă nu există evaluări
- IsoprenalineDocument2 paginiIsoprenalineImmanuel Victor GeorgeÎncă nu există evaluări
- TrihexyphenidylDocument7 paginiTrihexyphenidylfachsyarÎncă nu există evaluări
- Prozac (Fluoxetine) 40mgDocument1 paginăProzac (Fluoxetine) 40mgEÎncă nu există evaluări
- Clomipramine PDFDocument10 paginiClomipramine PDFDaniely RêgoÎncă nu există evaluări
- Drug OmeprazoleDocument1 paginăDrug OmeprazoleSrkocherÎncă nu există evaluări
- Isoprenaline Infusion 2016Document3 paginiIsoprenaline Infusion 2016Glory Claudia KarundengÎncă nu există evaluări
- TrazodoneDocument20 paginiTrazodoneAjay MehtaÎncă nu există evaluări
- DRUG-STUDY Butorphanol LRDR AngelicaRonquilloDocument2 paginiDRUG-STUDY Butorphanol LRDR AngelicaRonquillokarl eiron delos santosÎncă nu există evaluări
- Drug Classification: Antacid & Antihistamine Student ReportDocument2 paginiDrug Classification: Antacid & Antihistamine Student ReportKish AmoreÎncă nu există evaluări
- Generic Name TizanidineDocument3 paginiGeneric Name TizanidinemadamcloudnineÎncă nu există evaluări
- Generic Name: Mebeverine Hydrochloride Mechanism of Action Side Effects/ Adverse Reaction Nursing Responsibility Assessment & Drug EffectsDocument4 paginiGeneric Name: Mebeverine Hydrochloride Mechanism of Action Side Effects/ Adverse Reaction Nursing Responsibility Assessment & Drug EffectsNiziu BearsÎncă nu există evaluări
- StreptokinaseDocument8 paginiStreptokinaseemman_abzÎncă nu există evaluări
- College of Nursing: Cebu Normal UniversityDocument5 paginiCollege of Nursing: Cebu Normal UniversityChelsea WuÎncă nu există evaluări
- Methocarbamol (Robaxin)Document1 paginăMethocarbamol (Robaxin)EÎncă nu există evaluări
- Anxiolytic and Hypnotic AgentsDocument50 paginiAnxiolytic and Hypnotic AgentsMoxie Macado100% (1)
- Managing dextrose therapyDocument2 paginiManaging dextrose therapySanket TelangÎncă nu există evaluări
- Drug Study (MS)Document9 paginiDrug Study (MS)Kristine GallardoÎncă nu există evaluări
- DrugsDocument10 paginiDrugsRebecca JolieÎncă nu există evaluări
- Nursing Care Plan For Myocardial InfarctionDocument7 paginiNursing Care Plan For Myocardial InfarctionRocelyn CristobalÎncă nu există evaluări
- DobutamineDocument4 paginiDobutamineArvenaa Subramaniam100% (1)
- Acetazolamide Drug Study SummaryDocument4 paginiAcetazolamide Drug Study Summarygrail carantesÎncă nu există evaluări
- KetoconazoleDocument2 paginiKetoconazolenatinlalaÎncă nu există evaluări
- Fludrocortisone (Florinef)Document17 paginiFludrocortisone (Florinef)passer byÎncă nu există evaluări
- Cardiac Diet HandoutDocument2 paginiCardiac Diet Handoutapi-537434972Încă nu există evaluări
- Drug StudyDocument3 paginiDrug StudyKwin SaludaresÎncă nu există evaluări
- Premenstrual Dysphoric DisorderDocument11 paginiPremenstrual Dysphoric Disorderapi-3764215Încă nu există evaluări
- Case Pre Drug StudyDocument5 paginiCase Pre Drug StudyJoule PeirreÎncă nu există evaluări
- Drug Study Form TJDocument4 paginiDrug Study Form TJJasmin Santiago CarrilloÎncă nu există evaluări
- Alprazolam BiperidinDocument6 paginiAlprazolam BiperidinFionah RetuyaÎncă nu există evaluări
- DesyrelDocument1 paginăDesyrelKatie McPeekÎncă nu există evaluări
- Drug CelexaDocument1 paginăDrug CelexaSrkocher100% (1)
- Drug BisacodylDocument1 paginăDrug BisacodylSrkocherÎncă nu există evaluări
- Serratiopeptidase tablets effectively treat inflammationDocument12 paginiSerratiopeptidase tablets effectively treat inflammationdracula386Încă nu există evaluări
- DepakoteDocument2 paginiDepakotedana100% (1)
- DRUGSDocument5 paginiDRUGSDanica EspejoÎncă nu există evaluări
- Midazolam FinalDocument2 paginiMidazolam FinalAhmad AbqariÎncă nu există evaluări
- Drug Study..DokcyDocument7 paginiDrug Study..DokcyPeArl Peralta0% (1)
- Suxamethonium Chloride Injection BP Product Information SummaryDocument8 paginiSuxamethonium Chloride Injection BP Product Information SummarynanaÎncă nu există evaluări
- Albuterol, Accuneb Drug CardDocument2 paginiAlbuterol, Accuneb Drug Carddnw876Încă nu există evaluări
- Colestipol Hydrochloride Nursing ConsiderationsDocument3 paginiColestipol Hydrochloride Nursing ConsiderationsAbby AngÎncă nu există evaluări
- PrevacidDocument1 paginăPrevacidAdrianne BazoÎncă nu există evaluări
- Fluvastatin indications, contraindications, nursing responsibilitiesDocument1 paginăFluvastatin indications, contraindications, nursing responsibilitiesKevin H. MilanesÎncă nu există evaluări
- Valproic AcidDocument4 paginiValproic AcidAndrea Huecas TriaÎncă nu există evaluări
- 1678100677-2 - T20H0455 - SMPC - Approved - ReviewedDocument24 pagini1678100677-2 - T20H0455 - SMPC - Approved - ReviewedOmar Al-QadasiÎncă nu există evaluări
- Drugs Used in AneasthesiaDocument73 paginiDrugs Used in AneasthesiaCabdiladif Ahmed McrfÎncă nu există evaluări
- Drug Study LaderaDocument13 paginiDrug Study LaderaitheclubhunterÎncă nu există evaluări
- Critical care guidelines for IV nicardipine useDocument3 paginiCritical care guidelines for IV nicardipine useLisa Trisnawati ChaniagoÎncă nu există evaluări
- Drugstudy OrsdDocument10 paginiDrugstudy OrsdRafmar A. SalundaguitÎncă nu există evaluări
- Colorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsDocument48 paginiColorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsBrian HarrisÎncă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Colorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Document69 paginiColorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Brian HarrisÎncă nu există evaluări
- Colorado Medical Use of Marijuana Revised Statutes 18-18-406.3Document2 paginiColorado Medical Use of Marijuana Revised Statutes 18-18-406.3Brian HarrisÎncă nu există evaluări
- Colorado Medical Board Policy Guidelines For The Use of Controlled Substances For The Treatment of Pain 12-36-117, C.R.S.Document5 paginiColorado Medical Board Policy Guidelines For The Use of Controlled Substances For The Treatment of Pain 12-36-117, C.R.S.Brian HarrisÎncă nu există evaluări
- Colorado Peace Officer Manual 2013Document373 paginiColorado Peace Officer Manual 2013Brian Harris100% (1)
- Colorado Revised Statutes (CRS 12 12)Document65 paginiColorado Revised Statutes (CRS 12 12)Brian HarrisÎncă nu există evaluări
- Colorado Medical Use of Marijuana Department of Public Health and Environment Health and Environmental Information and Statistics Division 5 CCR 1006-2Document18 paginiColorado Medical Use of Marijuana Department of Public Health and Environment Health and Environmental Information and Statistics Division 5 CCR 1006-2Brian HarrisÎncă nu există evaluări
- Colorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Document69 paginiColorado CRS 18 18 - Uniform Controlled Substances Acto of 1992 Effective 7-1-2009Brian HarrisÎncă nu există evaluări
- Colorado Revised Statutes (CRS 12 36) Title 12 Article 36 and Article 36.5 Professions and Occupations, Medical Practice, Professional Review of Health Care ProvidersDocument57 paginiColorado Revised Statutes (CRS 12 36) Title 12 Article 36 and Article 36.5 Professions and Occupations, Medical Practice, Professional Review of Health Care ProvidersBrian HarrisÎncă nu există evaluări
- Colorado Preferred Drug List (PDL) 2013Document25 paginiColorado Preferred Drug List (PDL) 2013Brian HarrisÎncă nu există evaluări
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 paginiColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisÎncă nu există evaluări
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 paginiColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisÎncă nu există evaluări
- Colorado House Bill 11-1043 Concerning Medical Marijuana, and Making An Appropriation ThereforDocument24 paginiColorado House Bill 11-1043 Concerning Medical Marijuana, and Making An Appropriation ThereforBrian HarrisÎncă nu există evaluări
- Colorado Licensing of Controlled Substances Act 2013 Sunset ReviewDocument31 paginiColorado Licensing of Controlled Substances Act 2013 Sunset ReviewBrian HarrisÎncă nu există evaluări
- Colorado Guidelines of Professional Practice For Controlled Substances AddendumDocument14 paginiColorado Guidelines of Professional Practice For Controlled Substances AddendumBrian HarrisÎncă nu există evaluări
- Colorado Medical Board Policy Guidelines Pertaining To The Release and Retention of Medical Records Policy Number 40-07Document2 paginiColorado Medical Board Policy Guidelines Pertaining To The Release and Retention of Medical Records Policy Number 40-07Brian HarrisÎncă nu există evaluări
- Colorado Drug Control UpdateDocument7 paginiColorado Drug Control UpdateBrian HarrisÎncă nu există evaluări
- Colorado Guidelines of Professional Practice For Controlled Substances AddendumDocument14 paginiColorado Guidelines of Professional Practice For Controlled Substances AddendumBrian HarrisÎncă nu există evaluări
- Colorado Medical Marijuana Laws, Statutes, and CodesDocument60 paginiColorado Medical Marijuana Laws, Statutes, and CodesGreenpoint Insurance ColoradoÎncă nu există evaluări
- Medical Injuries or Illnesses To Use Medical Marijuana in ColoradoDocument5 paginiMedical Injuries or Illnesses To Use Medical Marijuana in ColoradoGreenpoint Insurance ColoradoÎncă nu există evaluări
- 42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleDocument28 pagini42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleBrian HarrisÎncă nu există evaluări
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 paginiColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisÎncă nu există evaluări
- ASAM The Role of The Physician in "Medical" MarijuanaDocument60 paginiASAM The Role of The Physician in "Medical" MarijuanaBrian HarrisÎncă nu există evaluări
- 42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleDocument28 pagini42 CFR Part 8 Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final RuleBrian HarrisÎncă nu există evaluări
- Alcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSDocument80 paginiAlcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSBrian HarrisÎncă nu există evaluări
- Colorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsDocument48 paginiColorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsBrian HarrisÎncă nu există evaluări
- The DEA Position On MarijuanaDocument63 paginiThe DEA Position On MarijuanaBrian HarrisÎncă nu există evaluări
- Pharmacist's Manual - An Information Outline of The Controlled Substances Act - 2010Document85 paginiPharmacist's Manual - An Information Outline of The Controlled Substances Act - 2010James LindonÎncă nu există evaluări
- Case PresentationDocument26 paginiCase Presentationfarhan yazdaniÎncă nu există evaluări
- Walgreens MTM PresentationDocument28 paginiWalgreens MTM Presentationtomoe hotaruÎncă nu există evaluări
- All by Gyn Obst Depart PDFDocument27 paginiAll by Gyn Obst Depart PDFRaouf Ra'fat Soliman100% (2)
- Dapus Episode 1Document6 paginiDapus Episode 1leny suardiÎncă nu există evaluări
- Team 9 SOPD Follow Up Recommendation and Operation GuidelineDocument7 paginiTeam 9 SOPD Follow Up Recommendation and Operation GuidelineChris Jardine LiÎncă nu există evaluări
- The Guardian - No. 54,260 (04 Feb 2021)Document64 paginiThe Guardian - No. 54,260 (04 Feb 2021)Adrian IonÎncă nu există evaluări
- Risk Factors Associated With Neonatal Jaundice: A Cross-Sectional Study From IranDocument7 paginiRisk Factors Associated With Neonatal Jaundice: A Cross-Sectional Study From Iranariani khikmatul mazidahÎncă nu există evaluări
- Parathyroid Carcinoma: Sudhir V Nair MS, MCH Associate Professor Head and Neck Oncosurgery Tata Memorial CenterDocument18 paginiParathyroid Carcinoma: Sudhir V Nair MS, MCH Associate Professor Head and Neck Oncosurgery Tata Memorial CenterSudhir NairÎncă nu există evaluări
- Anxiolytic, Sedative-Hypnotic DrugsDocument39 paginiAnxiolytic, Sedative-Hypnotic DrugsNina100% (1)
- Ebook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFDocument40 paginiEbook Egans Fundamentals of Respiratory Care 11Th Edition Kacmarek Test Bank Full Chapter PDFalexandercampbelldkcnzafgtw100% (8)
- Federal Regulations of Pressure Sores (F314Document3 paginiFederal Regulations of Pressure Sores (F314Jing CruzÎncă nu există evaluări
- 14 Drug StudyDocument15 pagini14 Drug StudyTricia AlvarezÎncă nu există evaluări
- Manual Lab Act Clinical Pathology-GUS-2021 FOR STUDENT 2122Document9 paginiManual Lab Act Clinical Pathology-GUS-2021 FOR STUDENT 2122EgieAprianÎncă nu există evaluări
- Sleep Disturbance: Esraa Albaqqal 371230183 Banin Alshehab 381230590 Yaqin Alkhalaf 391230503 Ahoud Alzaid 391230645Document14 paginiSleep Disturbance: Esraa Albaqqal 371230183 Banin Alshehab 381230590 Yaqin Alkhalaf 391230503 Ahoud Alzaid 391230645Banin malekÎncă nu există evaluări
- A MAN, GENRE APART: Dr. Avdhut BorkarDocument57 paginiA MAN, GENRE APART: Dr. Avdhut Borkarpediatric servicesÎncă nu există evaluări
- Rectal Cancer Partial VaginectomyDocument5 paginiRectal Cancer Partial VaginectomyArham ArsyadÎncă nu există evaluări
- Bed Sore Diagnosis and Treatment PlanningDocument2 paginiBed Sore Diagnosis and Treatment PlanningWyethBeltranDeLeonÎncă nu există evaluări
- Acute Flaccid Paralysis Case Investigation SummaryDocument1 paginăAcute Flaccid Paralysis Case Investigation SummarySerenity Zay'sÎncă nu există evaluări
- Spring / Summer 2011 Annual ReportDocument40 paginiSpring / Summer 2011 Annual ReportCCHSÎncă nu există evaluări
- Pediatrician Power Point 1Document11 paginiPediatrician Power Point 1Ashley100% (1)
- Medical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions ManualDocument8 paginiMedical Nutrition Therapy A Case Study Approach 5th Edition Nelms Solutions Manualsophiechaurfqnz100% (31)
- RH Factor PGDocument3 paginiRH Factor PGapi-375530349Încă nu există evaluări
- Valores Normales FanaroffDocument13 paginiValores Normales FanaroffLila Calapuja CalsinaÎncă nu există evaluări
- Adult Early Warning Score Observation Chart For Cardiology UnitDocument1 paginăAdult Early Warning Score Observation Chart For Cardiology UnitalexipsÎncă nu există evaluări
- Chinese Lunar Calendar Baby Gender Prediction MethodsDocument3 paginiChinese Lunar Calendar Baby Gender Prediction Methodsanand2k1Încă nu există evaluări
- Complete List of Subreddits To Build Drug Topic Corpus - JDI Supplementary MaterialDocument34 paginiComplete List of Subreddits To Build Drug Topic Corpus - JDI Supplementary MaterialJ CantuÎncă nu există evaluări
- Report ViewerDocument1 paginăReport ViewerHammad ur Rehman100% (1)
- Synopsis Proforma For Registration of Subject For DissertationDocument17 paginiSynopsis Proforma For Registration of Subject For Dissertationtanmai nooluÎncă nu există evaluări
- Family Medical TreeDocument2 paginiFamily Medical TreeDevi MayasariÎncă nu există evaluări
- ProPublica MethodologyDocument5 paginiProPublica MethodologySouthern California Public RadioÎncă nu există evaluări