S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- IER's National Physical Therapy Examination Review & Study Guide2 PDFDocument17 paginiIER's National Physical Therapy Examination Review & Study Guide2 PDFMhmd Iraky0% (1)
- Quadriplegia 2Document25 paginiQuadriplegia 2Mhmd IrakyÎncă nu există evaluări
- PPTDocument8 paginiPPTMhmd IrakyÎncă nu există evaluări
- PD Posture TreatmentDocument23 paginiPD Posture TreatmentMhmd IrakyÎncă nu există evaluări
- Brachial PlexopathyDocument14 paginiBrachial PlexopathyMhmd IrakyÎncă nu există evaluări
- Mid Level Paraplegia 4Document29 paginiMid Level Paraplegia 4Mhmd IrakyÎncă nu există evaluări
- Nerve InjuriesDocument68 paginiNerve InjuriesMhmd Iraky100% (1)
- NMJ DisordersDocument30 paginiNMJ DisordersMhmd IrakyÎncă nu există evaluări
- III. Mcqs NeuroDocument19 paginiIII. Mcqs NeuroMhmd Iraky100% (1)
- IV. Mcqs NeuroDocument7 paginiIV. Mcqs NeuroMhmd IrakyÎncă nu există evaluări
- Head Injuries 1Document15 paginiHead Injuries 1Mhmd IrakyÎncă nu există evaluări
- Low Level ParaplegiaDocument48 paginiLow Level ParaplegiaMhmd IrakyÎncă nu există evaluări
- I MCQs Neuro.Document4 paginiI MCQs Neuro.Mhmd Iraky100% (1)
- II. MCQs NeuroDocument13 paginiII. MCQs NeuroMhmd Iraky100% (2)
- Low Level ParaplegiaDocument86 paginiLow Level ParaplegiaMhmd IrakyÎncă nu există evaluări
- PT Residency BrochureDocument2 paginiPT Residency BrochureMhmd IrakyÎncă nu există evaluări
- Balance Assessment and TreatmentDocument55 paginiBalance Assessment and TreatmentMhmd Iraky100% (1)
- Motor Cortical AreasDocument2 paginiMotor Cortical AreasMhmd IrakyÎncă nu există evaluări
- Neuroanatomy MasterDocument49 paginiNeuroanatomy MasterMhmd IrakyÎncă nu există evaluări
- Balance Assessment and TreatmentDocument55 paginiBalance Assessment and TreatmentMhmd Iraky100% (1)
- ue 1-Broc s Are ʹ an area of the frontal lobe, usually in the left hemisphere, that directs the muscle movements involvedDocument31 paginiue 1-Broc s Are ʹ an area of the frontal lobe, usually in the left hemisphere, that directs the muscle movements involvedMhmd IrakyÎncă nu există evaluări
- Final Admissions ApplicationDocument6 paginiFinal Admissions ApplicationMhmd IrakyÎncă nu există evaluări
- Stroke Rehabilitation Conducted by PNF MethodDocument60 paginiStroke Rehabilitation Conducted by PNF MethodMhmd IrakyÎncă nu există evaluări
- Teaching Stroke ClassificationDocument24 paginiTeaching Stroke ClassificationBen omranÎncă nu există evaluări
- 640073resident ManualDocument45 pagini640073resident ManualMhmd IrakyÎncă nu există evaluări
- Internal Medicine Logbook ArabicDocument7 paginiInternal Medicine Logbook ArabicMhmd IrakyÎncă nu există evaluări
- Lesson Plan Info: #1Document4 paginiLesson Plan Info: #1sunshinegrlÎncă nu există evaluări
- Physical Therapy: PurposeDocument15 paginiPhysical Therapy: PurposeMhmd IrakyÎncă nu există evaluări
- NYS RequestforCredentialVerificationDocument1 paginăNYS RequestforCredentialVerificationMhmd IrakyÎncă nu există evaluări
- Curriculum Vitae: Victor F. Santamaria Gonzalez DOB: 01/16/1984 E-Mail: Phone Number: 541.346.0275Document3 paginiCurriculum Vitae: Victor F. Santamaria Gonzalez DOB: 01/16/1984 E-Mail: Phone Number: 541.346.0275Mhmd IrakyÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- American Journal of Occupational Therapy - 1Document13 paginiAmerican Journal of Occupational Therapy - 1TIMOTHY NYONGESAÎncă nu există evaluări
- The Terms Occupation and Activity Over The History of Official Occupational Therapy PublicationsDocument8 paginiThe Terms Occupation and Activity Over The History of Official Occupational Therapy PublicationsTO Joss AguilarÎncă nu există evaluări
- An Exploration of Addictive Behaviours From An Occupational PerspectiveDocument7 paginiAn Exploration of Addictive Behaviours From An Occupational PerspectiveFabricio Hernan Peralta BravoÎncă nu există evaluări
- Clinicians' Perceptions of The Benefits of Aquatic Therapy For Young Children With Autism A Preliminary StudyDocument10 paginiClinicians' Perceptions of The Benefits of Aquatic Therapy For Young Children With Autism A Preliminary Study黃安全Încă nu există evaluări
- Occupational Therapy in Sweden and Our Member AssociationDocument8 paginiOccupational Therapy in Sweden and Our Member AssociationRubilin NitishaÎncă nu există evaluări
- Mini Mental State Examination Cognitive FIM Instrument and The Loewenstein Occupational Therapy Cognitive Assessment Relation To Functional Outco PDFDocument4 paginiMini Mental State Examination Cognitive FIM Instrument and The Loewenstein Occupational Therapy Cognitive Assessment Relation To Functional Outco PDFDamira HalilovicÎncă nu există evaluări
- Evidence Table WorksheetDocument16 paginiEvidence Table Worksheetapi-282223043Încă nu există evaluări
- Spooner Pachana (2006)Document11 paginiSpooner Pachana (2006)CagolindaÎncă nu există evaluări
- Historical Perspective of NursingDocument6 paginiHistorical Perspective of NursingLove Jovellanos ÜÎncă nu există evaluări
- SJT Answers & RationaleDocument76 paginiSJT Answers & RationaleFarhan SakunÎncă nu există evaluări
- Leila Salhi ResumeDocument3 paginiLeila Salhi Resumeapi-547482419Încă nu există evaluări
- Pupil Support AssistantDocument10 paginiPupil Support AssistantLiam BaconÎncă nu există evaluări
- HC776Document4 paginiHC776Dawn CasuncadÎncă nu există evaluări
- Sensory Integration TherapyDocument7 paginiSensory Integration TherapyMárcia Ribeiro100% (1)
- Activity & Occupational AnalysisDocument6 paginiActivity & Occupational AnalysisZachary TagardaÎncă nu există evaluări
- Therapeutic Factors in Occupational Therapy GroupsDocument8 paginiTherapeutic Factors in Occupational Therapy Groupsthandiwebandile2Încă nu există evaluări
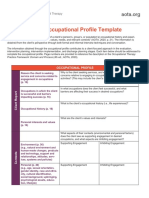
- AOTA Occupational Profile TemplateDocument2 paginiAOTA Occupational Profile Templatemelissa calabreseÎncă nu există evaluări
- Occupational Performance History Interview PDFDocument2 paginiOccupational Performance History Interview PDFBrad0% (4)
- Are Occupational Therapy Practitioners?: What, Why, Who, When, Where, and HowDocument2 paginiAre Occupational Therapy Practitioners?: What, Why, Who, When, Where, and HowGrace LÎncă nu există evaluări
- Cat Poster OfficialDocument1 paginăCat Poster Officialapi-292965056Încă nu există evaluări
- Andrews2000 The Value of Reflective Practice: A Student Case StudyDocument3 paginiAndrews2000 The Value of Reflective Practice: A Student Case StudyNatassa FerentinouÎncă nu există evaluări
- Willard and Spackman's Occupational Therapy 11th Edition Chapter 74 PDF FreeDocument25 paginiWillard and Spackman's Occupational Therapy 11th Edition Chapter 74 PDF FreeTracy NguyenÎncă nu există evaluări
- Dap NotesDocument2 paginiDap Notesapi-398892840Încă nu există evaluări
- Activities of Daily Living and Instrumental Activities of Daily LivingDocument17 paginiActivities of Daily Living and Instrumental Activities of Daily Livingjay soniÎncă nu există evaluări
- Final Eb ReflectionDocument2 paginiFinal Eb Reflectionapi-238460511Încă nu există evaluări
- II-Vocab of Hospital DeptDocument1 paginăII-Vocab of Hospital DeptAdhwaÎncă nu există evaluări
- OT Code of EthicsDocument8 paginiOT Code of Ethicsxarae23Încă nu există evaluări
- Occupational Therapy Using A Sensory Integration-Based Approach With Adult PopulationsDocument2 paginiOccupational Therapy Using A Sensory Integration-Based Approach With Adult PopulationsThe American Occupational Therapy Association75% (4)
- The Parents Guide To Occupational Therapy For Autism and Other Special Needs - NodrmDocument84 paginiThe Parents Guide To Occupational Therapy For Autism and Other Special Needs - NodrmAimeeUnidadEsguerra100% (1)
- Final Cat BaileysolheimDocument9 paginiFinal Cat Baileysolheimapi-314552584Încă nu există evaluări