S-ar putea să vă placă și
- Chicken Mole EnchiladasDocument2 paginiChicken Mole EnchiladasVanessa SantosÎncă nu există evaluări
- Asian Recipes - Dessert Delights (With I - Ho, CharlesDocument154 paginiAsian Recipes - Dessert Delights (With I - Ho, CharlesVanessa Santos100% (4)
- Chicken and Rice: IngredientsDocument1 paginăChicken and Rice: IngredientsVanessa SantosÎncă nu există evaluări
- Ps Calc GuideDocument30 paginiPs Calc GuideMzee321Încă nu există evaluări
- Personality Drawing TestDocument1 paginăPersonality Drawing TestVanessa SantosÎncă nu există evaluări
- Critical Care Calculations Study GuideDocument6 paginiCritical Care Calculations Study GuideAja Blue100% (2)
- Y Study CalculusDocument5 paginiY Study CalculusVanessa SantosÎncă nu există evaluări
- Characteristics of Greek LiteratureDocument2 paginiCharacteristics of Greek LiteratureVanessa Santos100% (2)
- 40 Items Comprehensive NCLEX ReviewDocument20 pagini40 Items Comprehensive NCLEX Reviewclumsy16Încă nu există evaluări
- A Spark of ExistenceDocument16 paginiA Spark of ExistenceVanessa SantosÎncă nu există evaluări
- Philippine Constitution PDFDocument53 paginiPhilippine Constitution PDFVanessa SantosÎncă nu există evaluări
- Personality Drawing TestDocument1 paginăPersonality Drawing TestVanessa SantosÎncă nu există evaluări
- Copar Final3Document4 paginiCopar Final3Vanessa SantosÎncă nu există evaluări
- Vs Circumference X 3.5Document1 paginăVs Circumference X 3.5Vanessa SantosÎncă nu există evaluări
- Common Communicable DiseasesDocument213 paginiCommon Communicable Diseasesɹǝʍdןnos100% (24)
- Acute Abdominal Pain and Acute AppendicitisDocument8 paginiAcute Abdominal Pain and Acute AppendicitisdrtpkÎncă nu există evaluări
- Republic Act No 9173Document5 paginiRepublic Act No 9173Vanessa SantosÎncă nu există evaluări
- Shock Case Presentation: General DataDocument1 paginăShock Case Presentation: General DataVanessa SantosÎncă nu există evaluări
- The CourtDocument6 paginiThe CourtVanessa SantosÎncă nu există evaluări
- GreekDocument7 paginiGreekVanessa SantosÎncă nu există evaluări
- LymphomaDocument15 paginiLymphomaVanessa SantosÎncă nu există evaluări
- IMCIDocument57 paginiIMCIwyndzÎncă nu există evaluări
- Spinal Disc HerniationDocument12 paginiSpinal Disc HerniationVanessa SantosÎncă nu există evaluări
- Adrenergic ReceptorsDocument6 paginiAdrenergic ReceptorsVanessa SantosÎncă nu există evaluări
- CDPDocument9 paginiCDPVanessa SantosÎncă nu există evaluări
- FractureDocument58 paginiFractureVanessa SantosÎncă nu există evaluări
- Stone LowOxalateDiet PDFDocument7 paginiStone LowOxalateDiet PDFVanessa Santos0% (1)
- IMCIDocument57 paginiIMCIwyndzÎncă nu există evaluări
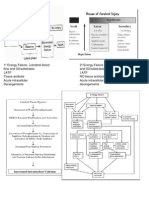
- 1º Energy FailureDocument1 pagină1º Energy FailureVanessa SantosÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- AllianzDocument27 paginiAllianzHariz SyahmiÎncă nu există evaluări
- Gestational Diabetes Mellitus: Science in MedicineDocument7 paginiGestational Diabetes Mellitus: Science in MedicinerizqarrÎncă nu există evaluări
- Guideline of Record-KeepingDocument9 paginiGuideline of Record-KeepingGen LCÎncă nu există evaluări
- Community Health Concepts NotesDocument7 paginiCommunity Health Concepts Noteswano chioneÎncă nu există evaluări
- Pendidikan Pasien Cath LabDocument10 paginiPendidikan Pasien Cath LabAgnesthesiaÎncă nu există evaluări
- Collaborative Practice Agreement 2024Document3 paginiCollaborative Practice Agreement 2024marlontapit1115Încă nu există evaluări
- Patheon Dosage CapabilitiesDocument6 paginiPatheon Dosage CapabilitiesHariharan90Încă nu există evaluări
- Preoperative Physiology, Imaging, andDocument13 paginiPreoperative Physiology, Imaging, andSiLfia SahrinÎncă nu există evaluări
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 paginiName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKarl Lourenz DeysolongÎncă nu există evaluări
- Congenital Anomalies: Dr. Bertha Soegiarto, Sp.ADocument26 paginiCongenital Anomalies: Dr. Bertha Soegiarto, Sp.AChristine VerinaÎncă nu există evaluări
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 paginăDepartment of Molecular Virology: COVID-19 (Corona) VirusHabib ur-RehmanÎncă nu există evaluări
- Stewardship White PaperDocument21 paginiStewardship White PaperHosam GomaaÎncă nu există evaluări
- Sepsis EncephalopathyDocument10 paginiSepsis EncephalopathyMarco Antonio KoffÎncă nu există evaluări
- Bowa Cat 10764 Electrosurgery Complete 2019 02 15 de en FR Es ItDocument208 paginiBowa Cat 10764 Electrosurgery Complete 2019 02 15 de en FR Es Itinstrumed_globalÎncă nu există evaluări
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 paginăCertificate For COVID-19 Vaccination: Beneficiary DetailsNikita KhjekarÎncă nu există evaluări
- 2022 AJOG A Laparoscopic Approach To Cesarean Scar Ectopic PregnancyDocument3 pagini2022 AJOG A Laparoscopic Approach To Cesarean Scar Ectopic PregnancyWilliam AlvarezÎncă nu există evaluări
- Chronic Lymphocytic Leukemia/ Small Lymphocytic LymphomaDocument84 paginiChronic Lymphocytic Leukemia/ Small Lymphocytic LymphomasimplyrosalynÎncă nu există evaluări
- ERASDocument39 paginiERASAnish H Dave100% (1)
- Askep Pada Acute Coronary Syndrome AcsDocument62 paginiAskep Pada Acute Coronary Syndrome Acsdefi rhÎncă nu există evaluări
- DPL OperationDocument2 paginiDPL OperationTao JunÎncă nu există evaluări
- MLSP111 PDF 03 - Professional Organizations PAMET PASMETH Schools of MTDocument6 paginiMLSP111 PDF 03 - Professional Organizations PAMET PASMETH Schools of MTANGELICA ROMAWAKÎncă nu există evaluări
- Gestational DiabetesDocument42 paginiGestational Diabetesjohn jumborock100% (1)
- Review Article: Phimosis in ChildrenDocument7 paginiReview Article: Phimosis in ChildrenmerlinÎncă nu există evaluări
- Cattle Diseases Farmers GuideDocument77 paginiCattle Diseases Farmers GuideDivyajyoti DevaÎncă nu există evaluări
- Clikstar Dispositivo Administrador InsulinaDocument11 paginiClikstar Dispositivo Administrador InsulinaHenry SilvaÎncă nu există evaluări
- Sample Care Coordination AgreementDocument2 paginiSample Care Coordination AgreementKristen LynchÎncă nu există evaluări
- Extraoral Radiography PDFDocument2 paginiExtraoral Radiography PDFJackÎncă nu există evaluări
- Urinalysis in Children and Adolescents, (2014)Document11 paginiUrinalysis in Children and Adolescents, (2014)Enrique MAÎncă nu există evaluări
- The Routes of Covid-19 Transmission: A Literature Review: Ati Surya Mediawati, Rachmat Susanto, Elly NurahmahDocument3 paginiThe Routes of Covid-19 Transmission: A Literature Review: Ati Surya Mediawati, Rachmat Susanto, Elly NurahmahChona Cari ReyesÎncă nu există evaluări
- Formula de PolloDocument8 paginiFormula de PolloYazmin Azucena Torres JuárezÎncă nu există evaluări