S-ar putea să vă placă și
- D TuningDocument2 paginiD TuningfreemedicÎncă nu există evaluări
- A Fieldbook of The StarsDocument130 paginiA Fieldbook of The StarsLiam Glen MurdochÎncă nu există evaluări
- C TuningDocument1 paginăC TuningfreemedicÎncă nu există evaluări
- World InstrumentsDocument2 paginiWorld InstrumentsfreemedicÎncă nu există evaluări
- DtuningDocument1 paginăDtuningtabayo_yatukishiÎncă nu există evaluări
- Chestsealinjury RevisedDocument20 paginiChestsealinjury RevisedfreemedicÎncă nu există evaluări
- Fleabag SongbookDocument14 paginiFleabag SongbookailopiÎncă nu există evaluări
- The Ukulele: A Magical History Tour: Bonus ChapterDocument2 paginiThe Ukulele: A Magical History Tour: Bonus Chapterfreemedic0% (1)
- Size of Tackle: The First Thing To Know Is What: OR LeatherDocument5 paginiSize of Tackle: The First Thing To Know Is What: OR Leatherelectricnusi100% (7)
- C TuningDocument1 paginăC TuningfreemedicÎncă nu există evaluări
- A Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentDocument6 paginiA Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentfreemedicÎncă nu există evaluări
- America's Greatest Special Ops Soldier: The Legend of Maj. Dick MeadowsDocument7 paginiAmerica's Greatest Special Ops Soldier: The Legend of Maj. Dick MeadowsfreemedicÎncă nu există evaluări
- Department of The Army Pyrotechnics Branch Aberdeen Proving Ground, Maryland 21020-5423Document5 paginiDepartment of The Army Pyrotechnics Branch Aberdeen Proving Ground, Maryland 21020-5423freemedicÎncă nu există evaluări
- Fleabag SongbookDocument14 paginiFleabag SongbookailopiÎncă nu există evaluări
- 6352 USN Phantoms in CombatDocument66 pagini6352 USN Phantoms in Combatfreemedic100% (16)
- TC3 GuidelinesDocument44 paginiTC3 Guidelinesfreemedic100% (1)
- Revisiting the James Black QuestionDocument17 paginiRevisiting the James Black QuestionfreemedicÎncă nu există evaluări
- Blood TransfusionDocument33 paginiBlood TransfusionfreemedicÎncă nu există evaluări
- TriageDocument6 paginiTriagefreemedicÎncă nu există evaluări
- Preserving meat without refrigeration through salting, smoking, drying and picklingDocument16 paginiPreserving meat without refrigeration through salting, smoking, drying and picklingfreemedic100% (2)
- Alss Aircrew Life SupportDocument74 paginiAlss Aircrew Life SupportfreemedicÎncă nu există evaluări
- My Survival Gear by Tom Tindell: Flint KitDocument3 paginiMy Survival Gear by Tom Tindell: Flint Kitfreemedic100% (1)
- BeretsDocument1 paginăBeretsfreemedic100% (1)
- Point North CatalogDocument84 paginiPoint North CatalogfreemedicÎncă nu există evaluări
- Soldiers of The Napoleonic Wars #4 - Colours and Weapons - British Foot Guards at Waterloo, June 1815Document26 paginiSoldiers of The Napoleonic Wars #4 - Colours and Weapons - British Foot Guards at Waterloo, June 1815J054663100% (7)
- Chapter 14Document32 paginiChapter 14freemedicÎncă nu există evaluări
- Eating AcornsDocument224 paginiEating Acornsapi-3707101100% (1)
- Woodsmoke Terms & Conditions for Overseas ExpeditionsDocument2 paginiWoodsmoke Terms & Conditions for Overseas ExpeditionsfreemedicÎncă nu există evaluări
- Chinook Cargo SystemDocument188 paginiChinook Cargo SystemfreemedicÎncă nu există evaluări
- Cold Water SurvivalDocument2 paginiCold Water SurvivalfreemedicÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Formal Report (Tests For Carbohydrates)Document15 paginiFormal Report (Tests For Carbohydrates)Angelo TolentinoÎncă nu există evaluări
- Your Peak Flow Diary PDFDocument11 paginiYour Peak Flow Diary PDFkalli987Încă nu există evaluări
- Syllabus-Advanced PhysiologyDocument4 paginiSyllabus-Advanced PhysiologyJa NetÎncă nu există evaluări
- Lactose intolerance diagnosis and treatmentDocument12 paginiLactose intolerance diagnosis and treatmentNico BatallaÎncă nu există evaluări
- Immediate Dentures by Me.Document59 paginiImmediate Dentures by Me.Mayura Badgujar100% (1)
- Module in Science 7: Department of Education Schools Division of Pasay CityDocument20 paginiModule in Science 7: Department of Education Schools Division of Pasay CityTorres Jhon Chriz GabrielÎncă nu există evaluări
- C C C C C C C C W C: Topic: Spiritual AssessmentDocument4 paginiC C C C C C C C W C: Topic: Spiritual AssessmentCacamo Rexell-anÎncă nu există evaluări
- Exam Stress: What Is It and How Can You Manage It?: Going and Focus On Your WorkDocument5 paginiExam Stress: What Is It and How Can You Manage It?: Going and Focus On Your WorkMahek PrakashÎncă nu există evaluări
- Thoracic Wall NotesDocument11 paginiThoracic Wall NotesAlfÎncă nu există evaluări
- BBC 17 12 PDFDocument40 paginiBBC 17 12 PDFLee-Ann LimÎncă nu există evaluări
- 4 Building A Fundation For Bagua - A Dynamic Stepping SystemDocument91 pagini4 Building A Fundation For Bagua - A Dynamic Stepping Systemvincraig100% (2)
- Citric Acid Cycle MCQsDocument15 paginiCitric Acid Cycle MCQsasjdg100% (2)
- Acfrogas81a C3gdggyv4xgrao Mdfic3te - x187f1 87lztljhozqte1uwyasvd30we4h6qfxqnls Kkx4fhvgdzsyhiidv6ruak2jsebl1ta-o6xhpricpgy55ribskr1dafecu67-RbikzqhDocument126 paginiAcfrogas81a C3gdggyv4xgrao Mdfic3te - x187f1 87lztljhozqte1uwyasvd30we4h6qfxqnls Kkx4fhvgdzsyhiidv6ruak2jsebl1ta-o6xhpricpgy55ribskr1dafecu67-RbikzqhSiseneg Tasma100% (1)
- Heart Arrhythmia GuideDocument77 paginiHeart Arrhythmia GuideSatria Pinandita100% (2)
- Ecg MDDocument121 paginiEcg MDdr. snehal patilÎncă nu există evaluări
- ACOSDocument14 paginiACOSDejan ŽujovićÎncă nu există evaluări
- Neuroimaging in Mild Traumatic Brain Injury: # Springer Science+Business Media, LLC 2010Document14 paginiNeuroimaging in Mild Traumatic Brain Injury: # Springer Science+Business Media, LLC 2010Sara Gonzalo RodríguezÎncă nu există evaluări
- Interpreting The Chest Radio Graph Friendly)Document9 paginiInterpreting The Chest Radio Graph Friendly)Vagner BorgesÎncă nu există evaluări
- Kinesiology of Shoulder Complex MusclesDocument7 paginiKinesiology of Shoulder Complex MusclesAlya Putri KhairaniÎncă nu există evaluări
- Aurora Poineeers Memeorial College Formerly: Cebuano Barracks Institute Aurora, Zamboanga Del Sur Final Examination College DepartmentDocument6 paginiAurora Poineeers Memeorial College Formerly: Cebuano Barracks Institute Aurora, Zamboanga Del Sur Final Examination College DepartmentEvaÎncă nu există evaluări
- Adaptogens: Herbs For Strength, Stamina, and Stress Relief - Updated & Expanded - 2nd EditionDocument7 paginiAdaptogens: Herbs For Strength, Stamina, and Stress Relief - Updated & Expanded - 2nd EditionSteven Maimes67% (3)
- Pulsus Paradoxus - Wikip PDFDocument4 paginiPulsus Paradoxus - Wikip PDFAniket MittalÎncă nu există evaluări
- Amaurosis FugaxDocument11 paginiAmaurosis FugaxRexArtem100% (1)
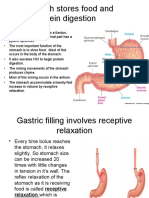
- Physiology, Lecture 8, GIT 2 (Stomach) (Slides)Document24 paginiPhysiology, Lecture 8, GIT 2 (Stomach) (Slides)Ali Al-Qudsi100% (2)
- Alice in IntensivelandDocument13 paginiAlice in IntensivelandPablo VélezÎncă nu există evaluări
- What Is NeurobicsDocument6 paginiWhat Is Neurobicsvarun_009Încă nu există evaluări
- New Born ExaminationDocument10 paginiNew Born ExaminationEn GeorgeÎncă nu există evaluări
- Biol 2334 - Molecular Biology Chapter 5 Worksheet - Replication & RepairDocument6 paginiBiol 2334 - Molecular Biology Chapter 5 Worksheet - Replication & RepairJohn Paradise100% (1)
- Solution Manual For Human Anatomy Laboratory Manual With Cat Dissections 7 e 7th EditionDocument9 paginiSolution Manual For Human Anatomy Laboratory Manual With Cat Dissections 7 e 7th EditionCristianRodriguezpawry100% (83)
- Test Bank For Principles of Anatomy and Physiology 15th Edition by TortoraDocument24 paginiTest Bank For Principles of Anatomy and Physiology 15th Edition by TortoraKennethGarciabqej100% (35)