S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- International System of UnitsDocument11 paginiInternational System of UnitsjbahalkehÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Inverse Function: DefinitionsDocument11 paginiInverse Function: Definitionsjbahalkeh100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Karl Marx Poverty of PhilosophyDocument84 paginiKarl Marx Poverty of PhilosophyjbahalkehÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Objective Plus Subjective Factors of Socialist RevolutionDocument13 paginiObjective Plus Subjective Factors of Socialist RevolutionjbahalkehÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Impact Factor Ranking JournalDocument2 paginiImpact Factor Ranking JournaljbahalkehÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Education: Early Years Arts and Sciences Bachelor in LebanonDocument6 paginiEducation: Early Years Arts and Sciences Bachelor in LebanonjbahalkehÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Maastricht Treaty: Navigation SearchDocument7 paginiMaastricht Treaty: Navigation SearchjbahalkehÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- 400 Bad Request 400 Bad Request Nginx/1.2.9Document128 pagini400 Bad Request 400 Bad Request Nginx/1.2.9jbahalkehÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- 400 Bad Request 400 Bad Request Nginx/1.2.9Document33 pagini400 Bad Request 400 Bad Request Nginx/1.2.9jbahalkehÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- 400 Bad Request 400 Bad Request Nginx/1.2.9Document48 pagini400 Bad Request 400 Bad Request Nginx/1.2.9jbahalkehÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Article Processing ChargesDocument4 paginiArticle Processing ChargesjbahalkehÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Ludwig WittgensteinDocument22 paginiLudwig WittgensteinjbahalkehÎncă nu există evaluări
- Occupation Military InterventionDocument24 paginiOccupation Military InterventionjbahalkehÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- 400 Bad Request 400 Bad Request Nginx/1.2.9Document209 pagini400 Bad Request 400 Bad Request Nginx/1.2.9jbahalkehÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Philippe Pétain and de GaulleDocument75 paginiPhilippe Pétain and de GaullejbahalkehÎncă nu există evaluări
- Layout - Foundation Drawing - Air BlowerDocument2 paginiLayout - Foundation Drawing - Air BlowerBabel THIAMÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- ABB Photovoltaic DisconnectorsDocument6 paginiABB Photovoltaic DisconnectorsBog PenÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- Amendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsDocument2 paginiAmendment No. 2 To AS 2047-2014 Windows and External Glazed Doors in BuildingsTommy AndersÎncă nu există evaluări
- IAL Hemanta Kumar KarDocument639 paginiIAL Hemanta Kumar KarTalita Abrani100% (4)
- Lesson 5 African LiteratureDocument3 paginiLesson 5 African LiteratureMiguel CarloÎncă nu există evaluări
- PRICELIST E Katalogs IVD 06042023 INDOPUTRA - PDF TerbaruDocument6 paginiPRICELIST E Katalogs IVD 06042023 INDOPUTRA - PDF Terbaruseksi sspk sarprasÎncă nu există evaluări
- Modeling and Simulation For Olefin Production in Amir Kabir PetrochemicalDocument7 paginiModeling and Simulation For Olefin Production in Amir Kabir PetrochemicalGhasem BashiriÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- BookDocument28 paginiBookFebrian Wardoyo100% (1)
- Notes On Peck&Coyle Practical CriticismDocument10 paginiNotes On Peck&Coyle Practical CriticismLily DameÎncă nu există evaluări
- Gayatri Mantras of Several GodDocument10 paginiGayatri Mantras of Several GodAnup KashyapÎncă nu există evaluări
- AsasDocument2 paginiAsasbuntu2003Încă nu există evaluări
- Air Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaDocument8 paginiAir Tunnels: Submitted By: Priyanka Sinha SK MD Sibli Akram Ananya Sreyansri NandaPriyanka SinhaÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Furuno FM 8700 Users Manual 429122Document102 paginiFuruno FM 8700 Users Manual 429122Igor MaranguanheÎncă nu există evaluări
- CR300 Wireless Communication ProtocolDocument130 paginiCR300 Wireless Communication ProtocolHenry Martinez BedoyaÎncă nu există evaluări
- Air Quality Index Analysis & PredictionDocument34 paginiAir Quality Index Analysis & PredictionGottumukkala Sravan KumarÎncă nu există evaluări
- Paper 1Document4 paginiPaper 1asa.henfield2Încă nu există evaluări
- 3 Particle Nature of Matter PDFDocument4 pagini3 Particle Nature of Matter PDFAtheer AlaniÎncă nu există evaluări
- Divine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionDocument2 paginiDivine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionNatasha VidhaniÎncă nu există evaluări
- Amos FortuneDocument97 paginiAmos Fortunetongai100% (5)
- Ferrozine Rapid Liquid Method Method 8147 0.009 To 1.400 MG/L Fe Pour-Thru CellDocument6 paginiFerrozine Rapid Liquid Method Method 8147 0.009 To 1.400 MG/L Fe Pour-Thru CellCarlos Andres MedinaÎncă nu există evaluări
- TNB Ar2011Document334 paginiTNB Ar2011Duncan LeeÎncă nu există evaluări
- A Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFDocument2 paginiA Bilateral Subdural Hematoma Case Report 2165 7548.1000112 PDFPutra GagahÎncă nu există evaluări
- Nelson Tables All in One PDFDocument618 paginiNelson Tables All in One PDFAmulya Ramakrishna100% (7)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
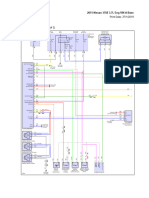
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDocument69 pagini2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaÎncă nu există evaluări
- Acid Alkaline Food ChartDocument3 paginiAcid Alkaline Food Chartgime2013Încă nu există evaluări
- Morality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordDocument3 paginiMorality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordTHEO DOMINIC REQUERME SILVOSAÎncă nu există evaluări
- Pipe Support Span CalculationDocument14 paginiPipe Support Span Calculationrajeevfa100% (3)
- BASIC ELECTRICAL MATERIALS AND METHODS - Specs - AllDocument202 paginiBASIC ELECTRICAL MATERIALS AND METHODS - Specs - AllAdnan NajemÎncă nu există evaluări
- German Din Vde Standards CompressDocument3 paginiGerman Din Vde Standards CompressYurii SlipchenkoÎncă nu există evaluări
- Manuel D'utilisation Maison AnglaisDocument17 paginiManuel D'utilisation Maison AnglaisVanesssÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 4.5 din 5 stele4.5/5 (82)