S-ar putea să vă placă și
- Atlas of Topographical and Pathotopographical Anatomy of the Head and NeckDe la EverandAtlas of Topographical and Pathotopographical Anatomy of the Head and NeckÎncă nu există evaluări
- Oral and Maxillofacial SurgeryDocument6 paginiOral and Maxillofacial Surgerysunaina chopraÎncă nu există evaluări
- Flint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsDocument20 paginiFlint Cumming Otolaryngology CHAPTER 93 - Odontogenesis Odontogenic Cysts and Odontogenic TumorsNicco Jake AlegroÎncă nu există evaluări
- ImpactionDocument11 paginiImpactionKhalid AgwaniÎncă nu există evaluări
- A Guide To Clinical Differential Diagnosis PDFDocument41 paginiA Guide To Clinical Differential Diagnosis PDFNisa Nafiah OktavianiÎncă nu există evaluări
- Essential Tissue Healing of the Face and NeckDe la EverandEssential Tissue Healing of the Face and NeckEvaluare: 5 din 5 stele5/5 (2)
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Seminar On Cleft Lip: Presented by DR - Cathrine Diana PG IIIDocument93 paginiSeminar On Cleft Lip: Presented by DR - Cathrine Diana PG IIIcareÎncă nu există evaluări
- Benign Non Odontogenic Tumors: Ossifying FibromaDocument10 paginiBenign Non Odontogenic Tumors: Ossifying FibromaIsabelle TanÎncă nu există evaluări
- Dental Caries: Cariology - MidtermsDocument29 paginiDental Caries: Cariology - MidtermskrstnkyslÎncă nu există evaluări
- Deep Vein Thrombosis in Oral and Maxillofacial Surgery-ADocument18 paginiDeep Vein Thrombosis in Oral and Maxillofacial Surgery-AMithun JithÎncă nu există evaluări
- Principles of Fixation For Maxillofacial Trauma PatientsDocument69 paginiPrinciples of Fixation For Maxillofacial Trauma PatientsSiyum MathewosÎncă nu există evaluări
- Oral Lichen PlanusDocument28 paginiOral Lichen PlanusParul SinghÎncă nu există evaluări
- Management of HIVHepatitis Patients in Oral and Maxillofacial SurgeryDocument6 paginiManagement of HIVHepatitis Patients in Oral and Maxillofacial Surgerymehak malhotraÎncă nu există evaluări
- Controversies in Condylar Fracture Repair UntalanDocument35 paginiControversies in Condylar Fracture Repair UntalanFrederick Mars Untalan100% (1)
- Prepostetic Surgery PDFDocument13 paginiPrepostetic Surgery PDFna zifaÎncă nu există evaluări
- Ectropion vs. EntropionDocument1 paginăEctropion vs. EntropionAhmed ShafikÎncă nu există evaluări
- Oral CancerDocument6 paginiOral CancerKedai ParentingÎncă nu există evaluări
- Flap SurgeryDocument61 paginiFlap SurgerySeptimiu TiplicaÎncă nu există evaluări
- Handout of Horizontal Jaw RelationsDocument12 paginiHandout of Horizontal Jaw RelationsPradusha RevuruÎncă nu există evaluări
- Chapter 24 Cysts of The Oral and Maxillofacial RegionDocument47 paginiChapter 24 Cysts of The Oral and Maxillofacial RegionJj JungÎncă nu există evaluări
- Zygomatic Bone FracturesDocument5 paginiZygomatic Bone FracturesAgung SajaÎncă nu există evaluări
- Aapd Guidelines - Restorative DentistryDocument8 paginiAapd Guidelines - Restorative DentistrymahmoudÎncă nu există evaluări
- Craniomaxillofacial Trauma: Tutorial of Basic SurgeryDocument42 paginiCraniomaxillofacial Trauma: Tutorial of Basic SurgeryShandy JonnerÎncă nu există evaluări
- Flaps in Maxillofacial ReconstructionDocument29 paginiFlaps in Maxillofacial ReconstructionJaspreet Kaur33% (3)
- Antibiotics in DentistryDocument3 paginiAntibiotics in DentistrymanikantatssÎncă nu există evaluări
- Module 6 Dr. AlbertoDocument10 paginiModule 6 Dr. AlbertoJASTHER LLOYD TOMANENGÎncă nu există evaluări
- Lesions of Oral CavityDocument43 paginiLesions of Oral CavityDawood NasserÎncă nu există evaluări
- Geriatric Dentistry NewDocument45 paginiGeriatric Dentistry NewRahul SinghÎncă nu există evaluări
- CANINE Impaction Oral SurgeryDocument64 paginiCANINE Impaction Oral SurgeryChampak PaulÎncă nu există evaluări
- Epidemiology of Oral Cancer PDFDocument6 paginiEpidemiology of Oral Cancer PDFمحمد عبدالهادي إسماعيلÎncă nu există evaluări
- ImpactionDocument167 paginiImpactionAME DENTAL COLLEGE RAICHUR, KARNATAKAÎncă nu există evaluări
- Oral Surgery in Pediatric DentistryDocument238 paginiOral Surgery in Pediatric Dentistrydrnadeemulla khan100% (1)
- Oral Surgery - Treatment Planning GuidelinesDocument5 paginiOral Surgery - Treatment Planning GuidelinesFaizal Prabowo KalimanÎncă nu există evaluări
- Risk Factors of Oral CancerDocument12 paginiRisk Factors of Oral CancerNauman ArshadÎncă nu există evaluări
- Epidemiologi Dental CariesDocument21 paginiEpidemiologi Dental CariesSampahAjaÎncă nu există evaluări
- Microvascular Free Flaps Used in Head and Neck Reconstruction. / Orthodontic Courses by Indian Dental AcademyDocument97 paginiMicrovascular Free Flaps Used in Head and Neck Reconstruction. / Orthodontic Courses by Indian Dental Academyindian dental academyÎncă nu există evaluări
- CH 30Document22 paginiCH 30Alejandra Oliveros VargasÎncă nu există evaluări
- Dental Considerations-CVS DiseasesDocument86 paginiDental Considerations-CVS Diseasesapi-3704106100% (1)
- Preprosthetic Surgery 12-02-015Document32 paginiPreprosthetic Surgery 12-02-015Yaser JasÎncă nu există evaluări
- Surgical EndoDocument16 paginiSurgical EndoTraian IlieÎncă nu există evaluări
- Premalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Document60 paginiPremalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Rajat NangiaÎncă nu există evaluări
- Chronic Vs Aggressive PeriodontitisDocument7 paginiChronic Vs Aggressive PeriodontitisSvnessa VanessaÎncă nu există evaluări
- Potentially Malignant Lesions and ConditionsDocument24 paginiPotentially Malignant Lesions and ConditionsNaleena Joseph100% (1)
- RPDDocument7 paginiRPDLea TomarongÎncă nu există evaluări
- Premalignant Conditions of The Oral Cavity: Peter A. Brennan Tom Aldridge Raghav C. Dwivedi EditorsDocument285 paginiPremalignant Conditions of The Oral Cavity: Peter A. Brennan Tom Aldridge Raghav C. Dwivedi EditorsShantanu DixitÎncă nu există evaluări
- Osteoradionecrosis CDEDocument32 paginiOsteoradionecrosis CDEYing Yi Teo100% (1)
- Diagnosis Word FPDDocument16 paginiDiagnosis Word FPDkaliapreetiÎncă nu există evaluări
- Panoramic RadiographDocument40 paginiPanoramic RadiographKelly YeowÎncă nu există evaluări
- PanoramikDocument38 paginiPanoramikStephanie Victoria100% (1)
- Mandibular Nerve BlockDocument32 paginiMandibular Nerve BlockVishesh JainÎncă nu există evaluări
- Management of Pediatric Mandible Fractures PDFDocument16 paginiManagement of Pediatric Mandible Fractures PDFarfahÎncă nu există evaluări
- Aggressive PeriodontitisDocument101 paginiAggressive Periodontitisdileep900100% (1)
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideDe la EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideÎncă nu există evaluări
- Wisdom Tooth WisdomDocument134 paginiWisdom Tooth WisdomPaulo Rabelo Jr.100% (1)
- Extraoral and Intraoral ExaminationDocument64 paginiExtraoral and Intraoral ExaminationAhmed HotiebaÎncă nu există evaluări
- Osteoradionecrosis of JawsDocument31 paginiOsteoradionecrosis of Jawsshagun singh100% (1)
- Gaint Cell Lesions UPLOADDocument176 paginiGaint Cell Lesions UPLOADAkshayÎncă nu există evaluări
- Surgical Complications of Minor Oral SurgeryDocument53 paginiSurgical Complications of Minor Oral SurgeryDrNagendra Dutt Sharma100% (1)
- Indication For Open Reduction of Condylar Fractures Zide and KentDocument10 paginiIndication For Open Reduction of Condylar Fractures Zide and Kentchanaish60% (1)
- ChemFil Superior44Document27 paginiChemFil Superior44محمد ابوالمجدÎncă nu există evaluări
- 4 3 937Document4 pagini4 3 937محمد ابوالمجدÎncă nu există evaluări
- VitaminsDocument13 paginiVitaminsمحمد ابوالمجدÎncă nu există evaluări
- Guidelines On Infection Control in Dental ClinicsDocument10 paginiGuidelines On Infection Control in Dental ClinicsHare RamÎncă nu există evaluări
- VitaminsDocument13 paginiVitaminsمحمد ابوالمجدÎncă nu există evaluări
- Biologic Width - The No Encroachment Zone: I J D ADocument8 paginiBiologic Width - The No Encroachment Zone: I J D AJinny ShawÎncă nu există evaluări
- Publication PDFDocument28 paginiPublication PDFمحمد ابوالمجدÎncă nu există evaluări
- Dental Anatomy DecksDocument362 paginiDental Anatomy Decksapi-2629165183% (6)
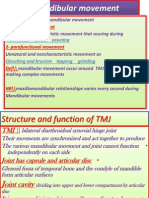
- Mandibular MovementDocument4 paginiMandibular Movementمحمد ابوالمجدÎncă nu există evaluări
- Dental Cements For UseDocument28 paginiDental Cements For UseAhmed DolaÎncă nu există evaluări
- Anatomy of CNSDocument32 paginiAnatomy of CNSLeonita AguillonÎncă nu există evaluări
- Serial Extraction PedoDocument23 paginiSerial Extraction PedoSelim BaftiuÎncă nu există evaluări
- Anatomy of CNSDocument32 paginiAnatomy of CNSLeonita AguillonÎncă nu există evaluări
- Publication PDFDocument20 paginiPublication PDFمحمد ابوالمجدÎncă nu există evaluări
- Behaviour Management 2Document59 paginiBehaviour Management 2Nikhil RaiÎncă nu există evaluări
- Finishing and PolishingDocument18 paginiFinishing and Polishingab0maiÎncă nu există evaluări
- Smear LayerDocument9 paginiSmear Layerpriyanka_gedamÎncă nu există evaluări
- Dental Management of Medically Compromised PatientsDocument12 paginiDental Management of Medically Compromised Patientsمحمد ابوالمجدÎncă nu există evaluări
- Emergency MedicineDocument7 paginiEmergency Medicineمحمد ابوالمجدÎncă nu există evaluări
- Mandibular MovementDocument4 paginiMandibular Movementمحمد ابوالمجدÎncă nu există evaluări
- Asnan 7 RulesDocument2 paginiAsnan 7 Rulesمحمد ابوالمجدÎncă nu există evaluări
- DentistryDocument71 paginiDentistryAnupama NagrajÎncă nu există evaluări
- Tooth MovementDocument14 paginiTooth Movementمحمد ابوالمجدÎncă nu există evaluări
- 1Document15 pagini1محمد ابوالمجدÎncă nu există evaluări
- Anatomy of CNSDocument32 paginiAnatomy of CNSLeonita AguillonÎncă nu există evaluări
- Etiology of MalocclusionDocument28 paginiEtiology of MalocclusionPriyaancaHaarsh100% (3)
- MCQSeptember 2006 Paper IDocument3 paginiMCQSeptember 2006 Paper Iapi-26291651100% (1)
- RO0111 00-00 WebberDocument6 paginiRO0111 00-00 WebberARTÎncă nu există evaluări
- OcclusionDocument17 paginiOcclusionمحمد ابوالمجدÎncă nu există evaluări
- MCQPaperSept 05Document4 paginiMCQPaperSept 05api-26291651100% (1)
- 100 Million Years of Food by Stephen LeDocument9 pagini100 Million Years of Food by Stephen Lesimas0% (1)
- Monday, October 06, 2014 EditionDocument12 paginiMonday, October 06, 2014 EditionFrontPageAfricaÎncă nu există evaluări
- Budgie Supplements & TreatmentsDocument5 paginiBudgie Supplements & TreatmentsAsafti AlinaÎncă nu există evaluări
- Applied Health Midterm Part II HL 250 JayDocument9 paginiApplied Health Midterm Part II HL 250 Jayapi-248193950Încă nu există evaluări
- Asthma: A. DefinitionDocument6 paginiAsthma: A. DefinitionElvando SimatupangÎncă nu există evaluări
- Oculofacial Plastic and Reconstructive SurgeryDocument562 paginiOculofacial Plastic and Reconstructive SurgeryGimena Dapena100% (3)
- Nursing Health Assessment Guide: San Pedro CollegeDocument3 paginiNursing Health Assessment Guide: San Pedro CollegeRue Cheng MaÎncă nu există evaluări
- 1000 MCQ Book Pain MedicineDocument215 pagini1000 MCQ Book Pain Medicineihtisham1100% (16)
- Drug-Food Interactions in Anti-Cancer TherapyDocument16 paginiDrug-Food Interactions in Anti-Cancer Therapyさゆう FayaÎncă nu există evaluări
- Internal Medicine 1, Conrad FischerDocument35 paginiInternal Medicine 1, Conrad Fischerdukelist566100% (3)
- Ebook - Minimal Intervention DentistrypdfDocument285 paginiEbook - Minimal Intervention DentistrypdfBerty SusantoÎncă nu există evaluări
- Chocolate: Prehrambeno-Tehnološki Fakultet Osijek Student: Maja GrgurovacDocument7 paginiChocolate: Prehrambeno-Tehnološki Fakultet Osijek Student: Maja GrgurovacMaja GrgurovacÎncă nu există evaluări
- PTBD 2Document4 paginiPTBD 2Alcntara AllenÎncă nu există evaluări
- Covid 19 Infographic enDocument1 paginăCovid 19 Infographic enTrilok AshpalÎncă nu există evaluări
- Chapter 3 - Microorganism in FoodDocument20 paginiChapter 3 - Microorganism in Foodnaa znlÎncă nu există evaluări
- AdrenalineDocument13 paginiAdrenalineMobahil AhmadÎncă nu există evaluări
- 1000 Plus Psychiatry MCQ Book DranilkakunjeDocument141 pagini1000 Plus Psychiatry MCQ Book Dranilkakunjethelegend 20220% (1)
- Assigmnt. On Cardiac RehabilitationDocument15 paginiAssigmnt. On Cardiac RehabilitationSachin Singh100% (1)
- 2013 ASA Guidelines Difficult AirwayDocument20 pagini2013 ASA Guidelines Difficult AirwayStacey WoodsÎncă nu există evaluări
- Essay 2 Working With Crisis and Trauma Draft 1 DO THHIS ONE Auto Saved) Auto Saved) Auto Saved)Document26 paginiEssay 2 Working With Crisis and Trauma Draft 1 DO THHIS ONE Auto Saved) Auto Saved) Auto Saved)Emily SummersÎncă nu există evaluări
- Scientific Career of Dr. Jaime Lagunez OteroDocument42 paginiScientific Career of Dr. Jaime Lagunez OteroFrente CivicoÎncă nu există evaluări
- Page From Thompson Thompson Genetics in Medicine 8Document2 paginiPage From Thompson Thompson Genetics in Medicine 8jorgegrodlÎncă nu există evaluări
- ExodontiaDocument32 paginiExodontiaahmed amerÎncă nu există evaluări
- Vinyl Chloride MonomerDocument6 paginiVinyl Chloride MonomerRizqia Putri ZakkaÎncă nu există evaluări
- Coding For SurgeonDocument379 paginiCoding For SurgeonLiza Fathiariani100% (1)
- 01-Hypro-Oss Clinical Assessment 2012 enDocument14 pagini01-Hypro-Oss Clinical Assessment 2012 enPaulus LagadanÎncă nu există evaluări
- 10 Herbal Plants Approved by Doh Herbs Indication PreparationDocument3 pagini10 Herbal Plants Approved by Doh Herbs Indication PreparationtatiÎncă nu există evaluări
- Resultados SaludDignaDocument2 paginiResultados SaludDignaAdriana RamosÎncă nu există evaluări
- Crisis ManagementDocument39 paginiCrisis ManagementbolutifeÎncă nu există evaluări