S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Instruments/ Assessments: AutismDocument27 paginiInstruments/ Assessments: AutismKadir Say'sÎncă nu există evaluări
- Anatomy & Physiology Bootcamp NotesDocument51 paginiAnatomy & Physiology Bootcamp Notesgeorgia robinsonÎncă nu există evaluări
- Clinical Examination and Applied Medicine, Volume I-Gastroenterology Series (Mar 7, 2018) - (1946646938) - (CRC Press)Document176 paginiClinical Examination and Applied Medicine, Volume I-Gastroenterology Series (Mar 7, 2018) - (1946646938) - (CRC Press)taher100% (1)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Asian Recipes - Dessert Delights (With I - Ho, CharlesDocument154 paginiAsian Recipes - Dessert Delights (With I - Ho, CharlesVanessa Santos100% (4)
- Cellular ResponsesDocument19 paginiCellular ResponsesFu Xiao ShanÎncă nu există evaluări
- Critical Care Calculations Study GuideDocument6 paginiCritical Care Calculations Study GuideAja Blue100% (2)
- British Biology Olympiad 2021Document66 paginiBritish Biology Olympiad 2021Yinyin ZhuÎncă nu există evaluări
- Mike Adams - The Healing Power of Sunlight Vitamin DDocument26 paginiMike Adams - The Healing Power of Sunlight Vitamin DJOSEPHÎncă nu există evaluări
- 978 0323049092 Color Textbook of Pediatric Dermatology Color Textbook of Pediatric Dermatology WestonDocument61 pagini978 0323049092 Color Textbook of Pediatric Dermatology Color Textbook of Pediatric Dermatology Westonaudrey.walston606100% (41)
- Characteristics of Greek LiteratureDocument2 paginiCharacteristics of Greek LiteratureVanessa Santos100% (2)
- Common Communicable DiseasesDocument213 paginiCommon Communicable Diseasesɹǝʍdןnos100% (24)
- Bone HealingDocument2 paginiBone HealingGerardLum100% (2)
- Drug Study For HepatitisDocument4 paginiDrug Study For Hepatitisunyokies100% (1)
- 40 Items Comprehensive NCLEX ReviewDocument20 pagini40 Items Comprehensive NCLEX Reviewclumsy16Încă nu există evaluări
- Personality Drawing TestDocument1 paginăPersonality Drawing TestVanessa SantosÎncă nu există evaluări
- Personality Drawing TestDocument1 paginăPersonality Drawing TestVanessa SantosÎncă nu există evaluări
- Chicken and Rice: IngredientsDocument1 paginăChicken and Rice: IngredientsVanessa SantosÎncă nu există evaluări
- Y Study CalculusDocument5 paginiY Study CalculusVanessa SantosÎncă nu există evaluări
- Ps Calc GuideDocument30 paginiPs Calc GuideMzee321Încă nu există evaluări
- Chicken Mole EnchiladasDocument2 paginiChicken Mole EnchiladasVanessa SantosÎncă nu există evaluări
- A Spark of ExistenceDocument16 paginiA Spark of ExistenceVanessa SantosÎncă nu există evaluări
- Philippine Constitution PDFDocument53 paginiPhilippine Constitution PDFVanessa SantosÎncă nu există evaluări
- Vs Circumference X 3.5Document1 paginăVs Circumference X 3.5Vanessa SantosÎncă nu există evaluări
- Copar Final3Document4 paginiCopar Final3Vanessa SantosÎncă nu există evaluări
- Republic Act No 9173Document5 paginiRepublic Act No 9173Vanessa SantosÎncă nu există evaluări
- Spinal Disc HerniationDocument12 paginiSpinal Disc HerniationVanessa SantosÎncă nu există evaluări
- IMCIDocument57 paginiIMCIwyndzÎncă nu există evaluări
- Shock Case Presentation: General DataDocument1 paginăShock Case Presentation: General DataVanessa SantosÎncă nu există evaluări
- Stone LowOxalateDiet PDFDocument7 paginiStone LowOxalateDiet PDFVanessa Santos0% (1)
- Acute Abdominal Pain and Acute AppendicitisDocument8 paginiAcute Abdominal Pain and Acute AppendicitisdrtpkÎncă nu există evaluări
- LymphomaDocument15 paginiLymphomaVanessa SantosÎncă nu există evaluări
- GreekDocument7 paginiGreekVanessa SantosÎncă nu există evaluări
- FractureDocument58 paginiFractureVanessa SantosÎncă nu există evaluări
- AgingDocument9 paginiAgingVanessa SantosÎncă nu există evaluări
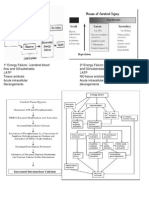
- 1º Energy FailureDocument1 pagină1º Energy FailureVanessa SantosÎncă nu există evaluări
- Adrenergic ReceptorsDocument6 paginiAdrenergic ReceptorsVanessa SantosÎncă nu există evaluări
- IMCIDocument57 paginiIMCIwyndzÎncă nu există evaluări
- CDPDocument9 paginiCDPVanessa SantosÎncă nu există evaluări
- Appl. Environ. Microbiol.-2011-Douglas-7365-71Document8 paginiAppl. Environ. Microbiol.-2011-Douglas-7365-71Nathan McCorkleÎncă nu există evaluări
- List+of+Greek+and+Latin+Roots+in+English+ +Wikipedia,+the+Free+EncyclopediaDocument46 paginiList+of+Greek+and+Latin+Roots+in+English+ +Wikipedia,+the+Free+EncyclopediaDyan SethupathiÎncă nu există evaluări
- 9700 m17 QP 22 PDFDocument16 pagini9700 m17 QP 22 PDFIG UnionÎncă nu există evaluări
- Application of Nanotechnology in PharmacyDocument13 paginiApplication of Nanotechnology in Pharmacykunasahu1Încă nu există evaluări
- Somatoform Disorder - DR - Ziad Arandi PowerpointDocument40 paginiSomatoform Disorder - DR - Ziad Arandi PowerpointNaji Z. ArandiÎncă nu există evaluări
- AlopeciaDocument10 paginiAlopeciaDr Vaishali MathapatiÎncă nu există evaluări
- Panayiotopoulos SyndromeDocument37 paginiPanayiotopoulos SyndromeZakaria MukallaÎncă nu există evaluări
- Amelogenesis Imperfecta Treatment Case ReviewDocument7 paginiAmelogenesis Imperfecta Treatment Case ReviewGeraldo LaurusÎncă nu există evaluări
- Legionella SPPDocument7 paginiLegionella SPPmtabatabaei20038889Încă nu există evaluări
- 9 JOHNSON BEHAVIOURAL SYSTEMfinalDocument11 pagini9 JOHNSON BEHAVIOURAL SYSTEMfinalRana VandanaÎncă nu există evaluări
- ArsenicDocument15 paginiArsenicIsabela PavălÎncă nu există evaluări
- CH 29Document39 paginiCH 29Jann Zaniel Allayne RiÎncă nu există evaluări
- Lactose Intolerance Pada AnakDocument11 paginiLactose Intolerance Pada AnakWilliam MakdinataÎncă nu există evaluări
- Bartonella in Benin 2016Document9 paginiBartonella in Benin 2016Yahya TfeilÎncă nu există evaluări
- HematDocument3 paginiHematMohit AbhyankarÎncă nu există evaluări
- Review: Lenat Joffe, Elena J LadasDocument11 paginiReview: Lenat Joffe, Elena J LadasGUSTAVO BELLOÎncă nu există evaluări
- 70791658786Document3 pagini70791658786gulcherrudisney259Încă nu există evaluări
- Public Speaking ScriptDocument2 paginiPublic Speaking Scriptsalbinarabi100% (1)
- Attention, Monotropism and Diagnosis Criteria For AutismDocument18 paginiAttention, Monotropism and Diagnosis Criteria For AutismyeyesÎncă nu există evaluări
- June 2016 (IAL) QP - Unit 3 Edexcel BiologyDocument16 paginiJune 2016 (IAL) QP - Unit 3 Edexcel BiologyRishita SinghÎncă nu există evaluări
- Biology Syllabus HSEBDocument2 paginiBiology Syllabus HSEBDipesh ShresthaÎncă nu există evaluări