S-ar putea să vă placă și
- Health HistoryDocument8 paginiHealth HistoryAhmed MohamedÎncă nu există evaluări
- The Turkey Book - An Introductory Manual For The WardsDocument147 paginiThe Turkey Book - An Introductory Manual For The WardsThe Physician Assistant LifeÎncă nu există evaluări
- Case Study FormatDocument4 paginiCase Study Formatapi-76740522Încă nu există evaluări
- Case Presentation Format 1Document4 paginiCase Presentation Format 1Ayessa Camelle DumileÎncă nu există evaluări
- Intro To Hcs Final Slo Review Answer KeyDocument7 paginiIntro To Hcs Final Slo Review Answer Keynurse1990Încă nu există evaluări
- PCM Guidebook For History Taking and Physical Exam, Revised Final, 9-20-17Document82 paginiPCM Guidebook For History Taking and Physical Exam, Revised Final, 9-20-17anon_925247980Încă nu există evaluări
- Soap 1Document26 paginiSoap 1sannnnrwa8Încă nu există evaluări
- 5th Year Study - Guide AUG 2017Document15 pagini5th Year Study - Guide AUG 2017Charity B JajiÎncă nu există evaluări
- Scare 2018 GuidelinesDocument2 paginiScare 2018 Guidelinesewqe100% (1)
- Oral Case Presentation Benchmarks - : Identifying Information & Chief ConcernDocument9 paginiOral Case Presentation Benchmarks - : Identifying Information & Chief ConcernManisanthosh KumarÎncă nu există evaluări
- Formal Patient Case Presentation FormatDocument2 paginiFormal Patient Case Presentation FormatMichael ChangÎncă nu există evaluări
- Case Study FormatDocument27 paginiCase Study FormatMarc Jamel ROdriguezÎncă nu există evaluări
- Getting the Most from Your Clinical ExperienceDocument52 paginiGetting the Most from Your Clinical ExperienceElise ChuaÎncă nu există evaluări
- How To Present A Patient CaseDocument4 paginiHow To Present A Patient CaseToni JÎncă nu există evaluări
- Medical Interview PrimerDocument8 paginiMedical Interview PrimerAlexÎncă nu există evaluări
- Language of Medici Ne: ODIADA, Eloisa Marie C. College of ArchitectureDocument30 paginiLanguage of Medici Ne: ODIADA, Eloisa Marie C. College of ArchitecturevevencioacuinÎncă nu există evaluări
- Universiti Kuala Lumpur Royal College of Medicine Perak: Year 3 Module Handbook (Medicine) 2014-2015Document15 paginiUniversiti Kuala Lumpur Royal College of Medicine Perak: Year 3 Module Handbook (Medicine) 2014-2015Codillia CheongÎncă nu există evaluări
- Medical Write Ups PPT Revised 4-20-10 2Document40 paginiMedical Write Ups PPT Revised 4-20-10 2AvinoamLuzonÎncă nu există evaluări
- Rle 106 ReqDocument10 paginiRle 106 Reqbeer_ettaaÎncă nu există evaluări
- Turkey BK 2013 - Full VersionDocument147 paginiTurkey BK 2013 - Full VersionmmmmzÎncă nu există evaluări
- A Road Map For The Soap Note-2021-2022: Name: DobDocument3 paginiA Road Map For The Soap Note-2021-2022: Name: DobDat Phan100% (1)
- Foundations of Clinical Medicine-1 Summer 2014 Semester: History TakingDocument63 paginiFoundations of Clinical Medicine-1 Summer 2014 Semester: History Takingparanoea911100% (1)
- Optometric Case AnalysisDocument93 paginiOptometric Case AnalysisJoseph IsraelÎncă nu există evaluări
- Case Study FormatDocument6 paginiCase Study FormatMark Jefferson LunaÎncă nu există evaluări
- Final Study Guide 2Document4 paginiFinal Study Guide 2Nataraj LoganathanÎncă nu există evaluări
- SCARE Checklist Case ReportDocument3 paginiSCARE Checklist Case ReportSylviany El Novita100% (1)
- Title 1 Key Words 2 3a: SCARE 2018 Checklist Topic Item Checklist Item Description NumberDocument5 paginiTitle 1 Key Words 2 3a: SCARE 2018 Checklist Topic Item Checklist Item Description NumberAmatystÎncă nu există evaluări
- Case Study Hospital FormatDocument3 paginiCase Study Hospital Formatsenyorakath0% (1)
- Resident Guide-Note Writing Inpatient Medicine WardsDocument10 paginiResident Guide-Note Writing Inpatient Medicine WardsGaetano Di GiovanniÎncă nu există evaluări
- Guide For Writing NotesDocument10 paginiGuide For Writing Notesiamsera100% (1)
- Scare - 2020 - Checklist SURGICAL CASES REPORTDocument7 paginiScare - 2020 - Checklist SURGICAL CASES REPORTBeni Bolng100% (1)
- 32 AN Guidelines H&PDocument3 pagini32 AN Guidelines H&Pabu alauon abed almohsenÎncă nu există evaluări
- Learning Description - Mallory CarterDocument7 paginiLearning Description - Mallory Carterapi-649060644Încă nu există evaluări
- How To Make An Oral Case Presentation To Healthcare ColleaguesDocument5 paginiHow To Make An Oral Case Presentation To Healthcare ColleaguesYuliana Citra AnggraeniÎncă nu există evaluări
- AVYKDocument6 paginiAVYKMinh Thành Trí LêÎncă nu există evaluări
- FORMAT (Case Study PPS 3)Document2 paginiFORMAT (Case Study PPS 3)Angel FiloteoÎncă nu există evaluări
- LMHI COVID-19 Clinical Case Report Submission FormDocument8 paginiLMHI COVID-19 Clinical Case Report Submission Formsamurai79Încă nu există evaluări
- The Art of Patient PresentationsDocument24 paginiThe Art of Patient Presentationsminerva_stanciuÎncă nu există evaluări
- Long Case Year 3 B2023Document41 paginiLong Case Year 3 B2023Mary AmeenÎncă nu există evaluări
- Dictation Discharge Summary TemplateDocument19 paginiDictation Discharge Summary TemplateBobby ReddyÎncă nu există evaluări
- Weekly Group Case Studies SOAP NotesDocument6 paginiWeekly Group Case Studies SOAP Notesmuhahss100% (1)
- Carte Semio Engl Modificata FinalDocument107 paginiCarte Semio Engl Modificata FinalMunteanu DragosÎncă nu există evaluări
- Case Study Format - PGTCNDocument2 paginiCase Study Format - PGTCNFitz JaminitÎncă nu există evaluări
- ReynoldsClinicalSkills CompleteHistoryChecklistDocument5 paginiReynoldsClinicalSkills CompleteHistoryChecklistCRUZ Jill EraÎncă nu există evaluări
- FNP Soap Note GuidelinesDocument6 paginiFNP Soap Note GuidelinesJosh Bat100% (1)
- Anglais 2022Document25 paginiAnglais 2022manelkandolo0818851800Încă nu există evaluări
- Root Cause Analysis PaDocument5 paginiRoot Cause Analysis PaStarr NewmanÎncă nu există evaluări
- History Taking - Progress NotesDocument21 paginiHistory Taking - Progress Notestwgp6pg5gh100% (1)
- The Oral PresentationDocument6 paginiThe Oral PresentationCarlos MellaÎncă nu există evaluări
- LBS CV Format 2014Document7 paginiLBS CV Format 2014Jonalyn Almuete RamosoÎncă nu există evaluări
- CARE Template PDFDocument2 paginiCARE Template PDFEduardo ArgüellesÎncă nu există evaluări
- Module 1 FOUNDATIONS OF CLINICAL PROFICIENCY PresentationDocument13 paginiModule 1 FOUNDATIONS OF CLINICAL PROFICIENCY Presentationdarius bautistaÎncă nu există evaluări
- Maharastra University of Health Sciences, Nashik: III M.B.B.S. MedicineDocument96 paginiMaharastra University of Health Sciences, Nashik: III M.B.B.S. Medicineanant_nimkar9243Încă nu există evaluări
- Future Doctor CCCDocument1 paginăFuture Doctor CCCwlshakespeareÎncă nu există evaluări
- MD (Hom.) Part-II Paediatrics syllabusDocument9 paginiMD (Hom.) Part-II Paediatrics syllabusDishaÎncă nu există evaluări
- Welcome Class of 2023 MB BS Internal Medicine Year 5Document184 paginiWelcome Class of 2023 MB BS Internal Medicine Year 5Ryubusa HayabusaÎncă nu există evaluări
- PAL Pack 2011 KI UpdateDocument41 paginiPAL Pack 2011 KI UpdateLuveon TangÎncă nu există evaluări
- H and P TemplateDocument6 paginiH and P Templatejhk0428100% (3)
- (Nursing English) DIYAH AHADYATUNNISADocument10 pagini(Nursing English) DIYAH AHADYATUNNISAdiyah hansuÎncă nu există evaluări
- The Nursing Management PROCESS: An Overview: Prof. Jhessie L. Abella, RN, RM, MANDocument30 paginiThe Nursing Management PROCESS: An Overview: Prof. Jhessie L. Abella, RN, RM, MANPrince Jhessie L. AbellaÎncă nu există evaluări
- Vernie Thesis ProposalDocument29 paginiVernie Thesis Proposaljonna mae talagsaÎncă nu există evaluări
- DLL - Mapeh 5 - Q3 - W5Document7 paginiDLL - Mapeh 5 - Q3 - W5Rodulfo Tortosa Paglomutan Jr.Încă nu există evaluări
- Rohini College CE6704 Unit V Report Preparation Lecture NotesDocument20 paginiRohini College CE6704 Unit V Report Preparation Lecture NotesRekhasreeGoneÎncă nu există evaluări
- Revised Academic Calender NITW 2011 2012Document2 paginiRevised Academic Calender NITW 2011 2012Sindhur GowravÎncă nu există evaluări
- Homework Does Not Increase Students' Potential in AcademicDocument10 paginiHomework Does Not Increase Students' Potential in AcademicNURIN HANISAH ZAINUL HISYAMÎncă nu există evaluări
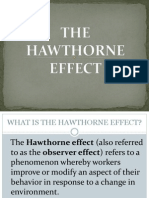
- The Hawthorne EffectDocument23 paginiThe Hawthorne EffectRishab MehraÎncă nu există evaluări
- CBLM Prepare and Serve Other Type of DessertsDocument7 paginiCBLM Prepare and Serve Other Type of DessertsLika Drin GabatinoÎncă nu există evaluări
- Reading Comprehension: The First Year of LifeDocument1 paginăReading Comprehension: The First Year of LifeViviana Elizabeth Cosme AriasÎncă nu există evaluări
- SOS in Software EngineeringDocument4 paginiSOS in Software EngineeringUltimate DiamondHeadÎncă nu există evaluări
- STATISTICDocument4 paginiSTATISTICCharlito PlasabasÎncă nu există evaluări
- Speaking Assessment at Secondary and Higher Secondary Levels and Students' Deficiency in Speaking Skill: A Study To Find InterdependenceDocument18 paginiSpeaking Assessment at Secondary and Higher Secondary Levels and Students' Deficiency in Speaking Skill: A Study To Find InterdependenceHana Mega LestariÎncă nu există evaluări
- A Qualitative Study of Health Information Seeking Behavior On The Internet Among Information Technology ProfessionalsDocument8 paginiA Qualitative Study of Health Information Seeking Behavior On The Internet Among Information Technology ProfessionalsYogesh BkÎncă nu există evaluări
- Protein Synthesis WorksheetDocument2 paginiProtein Synthesis WorksheetLovryan Tadena AmilingÎncă nu există evaluări
- Activity No.3-Problems and Obstacles To Economic Growth in Less Developed Countries-LOPEZ, JOEBIN C.Document1 paginăActivity No.3-Problems and Obstacles To Economic Growth in Less Developed Countries-LOPEZ, JOEBIN C.Joebin Corporal LopezÎncă nu există evaluări
- Totto Chan Book ReviewDocument1 paginăTotto Chan Book Reviewazie78Încă nu există evaluări
- Learning To Be DepressedDocument2 paginiLearning To Be Depressedapi-260339450Încă nu există evaluări
- Common GroundDocument2 paginiCommon GroundEmilyn Mae Nebril Perez100% (3)
- Analyzing Data Case StudiesDocument3 paginiAnalyzing Data Case StudiesankitaÎncă nu există evaluări
- Adult Learners InfographicDocument3 paginiAdult Learners Infographicapi-658327748Încă nu există evaluări
- Kenya Prisons Massive RecruitmentDocument1 paginăKenya Prisons Massive RecruitmentmohamedAmin Yussuf AbdiÎncă nu există evaluări
- Omega Psi PhiDocument20 paginiOmega Psi PhiScribdTranslationsÎncă nu există evaluări
- Assignment 1 OED (3 Abstracts and 1 Research Title)Document3 paginiAssignment 1 OED (3 Abstracts and 1 Research Title)Ezra Orita CeletariaÎncă nu există evaluări
- Chapter 1Document3 paginiChapter 1Merry Greece AyesÎncă nu există evaluări
- Unit 10 Language Focus (Đ T)Document27 paginiUnit 10 Language Focus (Đ T)Đạt PhạmÎncă nu există evaluări
- Overcoming Fear Impromptu SpeakingDocument6 paginiOvercoming Fear Impromptu SpeakingReymark TuanÎncă nu există evaluări
- Mandatory CLE requirements for Philippine lawyersDocument2 paginiMandatory CLE requirements for Philippine lawyersJana GreenÎncă nu există evaluări
- University Institute of Computing: Master of Computer Applications (MCA)Document8 paginiUniversity Institute of Computing: Master of Computer Applications (MCA)Rohit DahiyaÎncă nu există evaluări
- CW Week 6 Q2Document3 paginiCW Week 6 Q2Marky LoveÎncă nu există evaluări
- Interpersonal Skills ExercisesDocument25 paginiInterpersonal Skills Exercisesnitin2182295% (19)