S-ar putea să vă placă și
- Claim FormDocument3 paginiClaim FormRandy OrtonÎncă nu există evaluări
- IRDA Reimbursement Claim Form - InsuredDocument2 paginiIRDA Reimbursement Claim Form - InsuredSoham BanerjeeÎncă nu există evaluări
- Policy Schedule Two Wheeler-Cs2Document1 paginăPolicy Schedule Two Wheeler-Cs2Sunil NaikÎncă nu există evaluări
- AF - Sole and CAL BB DocusignDocument9 paginiAF - Sole and CAL BB DocusignManuel Castro IIÎncă nu există evaluări
- Contract: Buyer Details Organisation DetailsDocument4 paginiContract: Buyer Details Organisation DetailsAbhinn KothariÎncă nu există evaluări
- The New India Assurance Co. Ltd. (Government of India Undertaking)Document7 paginiThe New India Assurance Co. Ltd. (Government of India Undertaking)srikarÎncă nu există evaluări
- Information Report: in Respect of Article/Document Lost in Delhi SO No: 430/2014 Delhi PoliceDocument2 paginiInformation Report: in Respect of Article/Document Lost in Delhi SO No: 430/2014 Delhi PoliceSahil Ahmed JameiÎncă nu există evaluări
- Intermediary Code: Intermediary Name:: BR501650 Turtlemint Insurance Broking Service Private LimitedDocument2 paginiIntermediary Code: Intermediary Name:: BR501650 Turtlemint Insurance Broking Service Private LimitedAnuj bishtÎncă nu există evaluări
- UP78BU2412Document3 paginiUP78BU2412dushyant bhatnagar100% (1)
- Paramount Health Services & Insurance Tpa Private Limited: First Reminder Letter Without PrejudiceDocument1 paginăParamount Health Services & Insurance Tpa Private Limited: First Reminder Letter Without PrejudiceTanmoy Pal ChowdhuryÎncă nu există evaluări
- Sub:Risk Assumption Letter: Insured Vehicles DetailsDocument4 paginiSub:Risk Assumption Letter: Insured Vehicles Detailssumant samuelÎncă nu există evaluări
- Final Motor Insurance Claim Form Two Aug2018 - 0 PDFDocument1 paginăFinal Motor Insurance Claim Form Two Aug2018 - 0 PDFShiva SinghÎncă nu există evaluări
- InvoiceDocument1 paginăInvoiceRadheshyam SinghÎncă nu există evaluări
- Go Digit General Insurance LTD.: IRDAN158RP0003V01201718Document2 paginiGo Digit General Insurance LTD.: IRDAN158RP0003V01201718sarath potnuriÎncă nu există evaluări
- The Oriental Insurance Company LimitedDocument3 paginiThe Oriental Insurance Company LimitedrituÎncă nu există evaluări
- Future Generali India: Insurance Company LimitedDocument2 paginiFuture Generali India: Insurance Company Limitedstar pandiÎncă nu există evaluări
- Bajaj AllianzDocument2 paginiBajaj AllianzKashish BangaloreÎncă nu există evaluări
- CNandReceiptWaterMark 1403789874695Document3 paginiCNandReceiptWaterMark 1403789874695Liau Siew Ling0% (1)
- Policy No 26020531196210020451 Proposal No. & Date Policy Issued On Period of Insurance Insured Name Previous Policy No. Insured Add Previous InsurerDocument2 paginiPolicy No 26020531196210020451 Proposal No. & Date Policy Issued On Period of Insurance Insured Name Previous Policy No. Insured Add Previous InsurerSanjay SharmaÎncă nu există evaluări
- Tnvat Form WW Fy 15-16Document30 paginiTnvat Form WW Fy 15-16samaadhuÎncă nu există evaluări
- Ac Ko Ac Ko Advant Ag e Advant Ag eDocument6 paginiAc Ko Ac Ko Advant Ag e Advant Ag eJeet TrivediÎncă nu există evaluări
- Star CityDocument1 paginăStar CityAjai K0% (1)
- Auto Secure Private Car Package PolicyDocument6 paginiAuto Secure Private Car Package PolicyAbhishek Apoorva ApoorvaÎncă nu există evaluări
- HDFC Ergo Policy ScheduleDocument3 paginiHDFC Ergo Policy ScheduleReshma GuptaÎncă nu există evaluări
- Form 2 (See Rules 10, 14, 17 and 18)Document8 paginiForm 2 (See Rules 10, 14, 17 and 18)Aastik AggarwalÎncă nu există evaluări
- Upes Fee Invoice PDFDocument1 paginăUpes Fee Invoice PDFJai SingalÎncă nu există evaluări
- Form 28 - Application For RTO NOCDocument2 paginiForm 28 - Application For RTO NOCspirit3189Încă nu există evaluări
- Ahmed BashaDocument1 paginăAhmed BashaYASHÎncă nu există evaluări
- CPOLICYdoc 01050048194100210965 PDFDocument2 paginiCPOLICYdoc 01050048194100210965 PDFTanish MaanÎncă nu există evaluări
- Agent Name Khivraj Motors Agent Code MIS1000132 Agent Contact No 9108694880Document2 paginiAgent Name Khivraj Motors Agent Code MIS1000132 Agent Contact No 9108694880SanthoshÎncă nu există evaluări
- Motor Policy Schedule Cum Certificate of InsuranceDocument2 paginiMotor Policy Schedule Cum Certificate of InsurancePRAVIN MYAKALWAR100% (1)
- Vrpower Equipments PVT LTD BhartiDocument8 paginiVrpower Equipments PVT LTD BhartiMADHUKAR JHANKALÎncă nu există evaluări
- Acko All-Round Protection PlanDocument4 paginiAcko All-Round Protection PlanrahilkelaÎncă nu există evaluări
- FTA HSRP SoDocument1 paginăFTA HSRP SoAnkit RupaparaÎncă nu există evaluări
- Commercial Vehicle Package Policy-5Document3 paginiCommercial Vehicle Package Policy-5Sunil KumarÎncă nu există evaluări
- Motor Insurance Certificate Cum Policy Schedule Motorised-Two Wheelers Liability Only Policy - Zone BDocument4 paginiMotor Insurance Certificate Cum Policy Schedule Motorised-Two Wheelers Liability Only Policy - Zone BRaghunandan R'dyÎncă nu există evaluări
- Application No. 2105 2013 7035: UGC-NET December 2020 and June 2021 CyclesDocument1 paginăApplication No. 2105 2013 7035: UGC-NET December 2020 and June 2021 CyclesMantasha KhanÎncă nu există evaluări
- Reliance General Insurance Company Limited: Reliance Two Wheeler Package Policy-BundledDocument6 paginiReliance General Insurance Company Limited: Reliance Two Wheeler Package Policy-Bundledu want some then come and get someÎncă nu există evaluări
- Mohit Agarwal: Raipur Pin Code - 492001 (C.G.)Document1 paginăMohit Agarwal: Raipur Pin Code - 492001 (C.G.)Bunny PatelÎncă nu există evaluări
- Reliance Mutual Funds Compelete Application FormDocument10 paginiReliance Mutual Funds Compelete Application FormARVINDÎncă nu există evaluări
- Form 10 DDocument6 paginiForm 10 DilyaskureshiÎncă nu există evaluări
- Sareen C K Bike InsuranceDocument1 paginăSareen C K Bike InsurancesareenckÎncă nu există evaluări
- keyFactStatement PDFDocument8 paginikeyFactStatement PDFINAM JUNG GUJJARÎncă nu există evaluări
- M3L2Document4 paginiM3L2ajayroy12Încă nu există evaluări
- HR Baby Coil 16-12-2019 - 62983 - 1.10 PDFDocument19 paginiHR Baby Coil 16-12-2019 - 62983 - 1.10 PDFsoumya palÎncă nu există evaluări
- Shamse Alam PDFDocument4 paginiShamse Alam PDFaxis motorsÎncă nu există evaluări
- Vendor Registration Form - FKF1J.v2Document2 paginiVendor Registration Form - FKF1J.v2Ryzen AnimationÎncă nu există evaluări
- Insurance Copy Activa 1255 PDFDocument4 paginiInsurance Copy Activa 1255 PDFDivya SuvarnaÎncă nu există evaluări
- Fee Letter - 1010Document1 paginăFee Letter - 1010Manoj KumarÎncă nu există evaluări
- Fsec & Fsic Application Form 2020Document2 paginiFsec & Fsic Application Form 2020Shi Yuan ZhangÎncă nu există evaluări
- Generic Travel Expense ReportDocument1 paginăGeneric Travel Expense ReportXYZÎncă nu există evaluări
- Income Tax Refund RTI ApplicationDocument3 paginiIncome Tax Refund RTI Applicationcharul.shukla100% (2)
- Policy No 3005 - 117287654 - 01 - 000Document3 paginiPolicy No 3005 - 117287654 - 01 - 000Prakash ChoudharyÎncă nu există evaluări
- Account Statement 1649661081074Document2 paginiAccount Statement 1649661081074manas trivediÎncă nu există evaluări
- The Oriental Insurance Company LimitedDocument3 paginiThe Oriental Insurance Company LimitedDibya DillipÎncă nu există evaluări
- Xuv Up 16 Ar 2053Document3 paginiXuv Up 16 Ar 2053luckandhardÎncă nu există evaluări
- Employment Pass / S Pass Appeal FormDocument7 paginiEmployment Pass / S Pass Appeal FormjoegrantosÎncă nu există evaluări
- 31 2020 1571 PDFDocument2 pagini31 2020 1571 PDFNandakishor AjÎncă nu există evaluări
- Motor Claim FormDocument3 paginiMotor Claim FormjavednjavedÎncă nu există evaluări
- Marine Cargo Claim FormDocument4 paginiMarine Cargo Claim FormtbalaÎncă nu există evaluări
- Satisfactory VoucherDocument1 paginăSatisfactory Vouchervrevatienterprises100% (2)
- Star Mer FormDocument4 paginiStar Mer FormvrevatienterprisesÎncă nu există evaluări
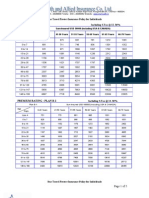
- Individual Travel Protect Premium Chart ST 12.36%Document5 paginiIndividual Travel Protect Premium Chart ST 12.36%vrevatienterprisesÎncă nu există evaluări
- Shriram Claim FormDocument2 paginiShriram Claim FormvrevatienterprisesÎncă nu există evaluări
- Corporate Reporting Paper 3 1 May2018Document26 paginiCorporate Reporting Paper 3 1 May2018financial reportingÎncă nu există evaluări
- Warrantage of Agricultural ProductDocument47 paginiWarrantage of Agricultural Productandysupa100% (1)
- Advanced Accounting Baker Test Bank - Chap008Document35 paginiAdvanced Accounting Baker Test Bank - Chap008donkazotey100% (5)
- Accounting Problem Book 2011 PDFDocument103 paginiAccounting Problem Book 2011 PDFViệt Đức Lê67% (3)
- Professional EnglishDocument10 paginiProfessional EnglishFrancesca Rutti AlvaradoÎncă nu există evaluări
- Ka Samba HayDocument39 paginiKa Samba HayMarvin ChuaÎncă nu există evaluări
- 50-30-20 Budget TemplateDocument1 pagină50-30-20 Budget TemplateKhairul IkhwanÎncă nu există evaluări
- TemplateDocument3 paginiTemplatekilokane100% (15)
- Request A Lending and Leasing As A Service BrochureDocument3 paginiRequest A Lending and Leasing As A Service BrochureFahim ChougleÎncă nu există evaluări
- Dudh Sagar Dairy of Financial ReportDocument83 paginiDudh Sagar Dairy of Financial ReportPatel Kashyap100% (2)
- Toys "R" Us, Inc.: United States Securities and Exchange Commission FORM 10-QDocument38 paginiToys "R" Us, Inc.: United States Securities and Exchange Commission FORM 10-QAdam Miguel LopezÎncă nu există evaluări
- Chapter - 1Document88 paginiChapter - 1Masudur Rahman0% (1)
- RatiosDocument12 paginiRatiosstuck00123Încă nu există evaluări
- Corporate Restructuring Under Insolvency and Bankruptcy Code 2016Document21 paginiCorporate Restructuring Under Insolvency and Bankruptcy Code 2016Manish SinghÎncă nu există evaluări
- Continuous Time Finance: Tomas BJ Ork Stockholm School of EconomicsDocument387 paginiContinuous Time Finance: Tomas BJ Ork Stockholm School of Economicsjavi_doggÎncă nu există evaluări
- A Project Report ON: Working Capital ManagementDocument44 paginiA Project Report ON: Working Capital ManagementShubham More CenationÎncă nu există evaluări
- Ratio Analysis of Engro Vs NestleDocument24 paginiRatio Analysis of Engro Vs NestleMuhammad SalmanÎncă nu există evaluări
- Cheque Mate Game Current (Tran Code 11) (Tran Code 29) Saving (Tran Code 10) HNI (Tran Code 31)Document1 paginăCheque Mate Game Current (Tran Code 11) (Tran Code 29) Saving (Tran Code 10) HNI (Tran Code 31)Nandini JaganÎncă nu există evaluări
- Asynchronous Class Questions To Answer and Reason Why You Choose Such AnswerDocument9 paginiAsynchronous Class Questions To Answer and Reason Why You Choose Such Answerangelo eleazarÎncă nu există evaluări
- Chapter 15 Q&PDocument49 paginiChapter 15 Q&PPramod KumawatÎncă nu există evaluări
- 3.3 Instalment PurchasedDocument4 pagini3.3 Instalment PurchasedharizÎncă nu există evaluări
- Interrogatories Directed at American Express Centurion BankDocument5 paginiInterrogatories Directed at American Express Centurion Bankluke17Încă nu există evaluări
- 1Document79 pagini1AnthonyÎncă nu există evaluări
- Revision For The Final Exam (With Results) : Instructor: Course: SemesterDocument12 paginiRevision For The Final Exam (With Results) : Instructor: Course: SemesterashibhallauÎncă nu există evaluări
- Guarantor FormDocument2 paginiGuarantor FormRadiantGoddess100% (3)
- UP08 Commercial LawDocument351 paginiUP08 Commercial LawsufistudentÎncă nu există evaluări
- A. Methodology: Condominium ActDocument13 paginiA. Methodology: Condominium ActPrei BaltazarÎncă nu există evaluări
- A151 Tutorial Topic 5 - QuestionDocument3 paginiA151 Tutorial Topic 5 - QuestionNadirah Mohamad Sarif100% (1)
- AccountsDocument5 paginiAccountsAlyssa CasimiroÎncă nu există evaluări
- Financial Management September 2013 Mark Plan ICAEW PDFDocument9 paginiFinancial Management September 2013 Mark Plan ICAEW PDFMuhammad Ziaul HaqueÎncă nu există evaluări