S-ar putea să vă placă și
- AAE Newsletter Covers Endodontic TreatmentDocument6 paginiAAE Newsletter Covers Endodontic TreatmentMehwish MunawarÎncă nu există evaluări
- Case Selection in Dental Implant TherapyDocument4 paginiCase Selection in Dental Implant Therapymichealraj rousseauÎncă nu există evaluări
- Adjuncts to Mouth Reconstruction TechniquesDocument5 paginiAdjuncts to Mouth Reconstruction TechniquesAmar BhochhibhoyaÎncă nu există evaluări
- Andersson 2003Document6 paginiAndersson 2003IngrydCamposÎncă nu există evaluări
- JC 2 A RefDocument5 paginiJC 2 A RefHarish Kumar.THOTAÎncă nu există evaluări
- Internet-Based Prevention: Monitoring ToothbrushingDocument3 paginiInternet-Based Prevention: Monitoring ToothbrushingoanaÎncă nu există evaluări
- Restoring Endodontically Treated TeethDocument20 paginiRestoring Endodontically Treated Teethlishenwong100% (1)
- JCDP 20 1108Document10 paginiJCDP 20 1108snkidÎncă nu există evaluări
- D L, H R & L L: Periodontology 2000Document24 paginiD L, H R & L L: Periodontology 2000ph4nt0mgr100% (1)
- Current Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDocument10 paginiCurrent Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDONGXU LIUÎncă nu există evaluări
- PCSO Fall - 10 Seasoned Practitioner's CornerDocument5 paginiPCSO Fall - 10 Seasoned Practitioner's CornerDame rohanaÎncă nu există evaluări
- ORTHO - Treatment Planning and Management of Class I MalocclusionDocument31 paginiORTHO - Treatment Planning and Management of Class I MalocclusionLailathul Bathur Kalikul Jaman50% (2)
- JCDP 22 1135Document9 paginiJCDP 22 1135Thang Nguyen TienÎncă nu există evaluări
- Clinical Longevity of Removable Partial Dentures Retained by Telescopic Crowns: Outcome of The Double Crown With Clearance FitDocument8 paginiClinical Longevity of Removable Partial Dentures Retained by Telescopic Crowns: Outcome of The Double Crown With Clearance FitStephanie NúñezÎncă nu există evaluări
- Challenges in Trophivc MandibleDocument4 paginiChallenges in Trophivc MandibleAshish PandaÎncă nu există evaluări
- Endodontic Case Complexity and Working With The Specialist No VoiceDocument14 paginiEndodontic Case Complexity and Working With The Specialist No VoiceLinh PhanÎncă nu există evaluări
- PEAK Restoration of The Endodontically Treated Tooth PDFDocument20 paginiPEAK Restoration of The Endodontically Treated Tooth PDFana9025100% (1)
- Extraction Planningin OrthodonticsDocument6 paginiExtraction Planningin OrthodonticsAdina SerbanÎncă nu există evaluări
- Systematic Review On Sucess of Narrow-Diameter Dental ImplantsDocument37 paginiSystematic Review On Sucess of Narrow-Diameter Dental ImplantsMaryGonzalesʚïɞÎncă nu există evaluări
- Three-Dimensional Soft Tissue Evaluation After Rapid Maxillary Expansion and Mandibular Midline Distraction OsteogenesisDocument7 paginiThree-Dimensional Soft Tissue Evaluation After Rapid Maxillary Expansion and Mandibular Midline Distraction OsteogenesisayisÎncă nu există evaluări
- 1 s2.0 S001185321830096X MainDocument16 pagini1 s2.0 S001185321830096X MainSeto PÎncă nu există evaluări
- Pulpotomy For Treatment of Complicated Crown FracturesDocument22 paginiPulpotomy For Treatment of Complicated Crown Fracturessystematic reviewÎncă nu există evaluări
- Endodontic ArmamentariumDocument29 paginiEndodontic ArmamentariumAbdulSamiÎncă nu există evaluări
- 1 s2.0 S0889540616001955 MainDocument9 pagini1 s2.0 S0889540616001955 MainPanaite TinelaÎncă nu există evaluări
- Dental Implants With Fixed Prosthodontics in Oligodontia A Retrospective Cohort StudyDocument7 paginiDental Implants With Fixed Prosthodontics in Oligodontia A Retrospective Cohort StudyfghdhmdkhÎncă nu există evaluări
- Mesodens AutotransplantDocument9 paginiMesodens Autotransplantnandani kumariÎncă nu există evaluări
- Retrospective Study On Efficacy of Intermaxillary Fixation ScrewsDocument3 paginiRetrospective Study On Efficacy of Intermaxillary Fixation ScrewsPorcupine TreeÎncă nu există evaluări
- Surgical Guidelines For Dental Implant Placement: British Dental Journal September 2006Document15 paginiSurgical Guidelines For Dental Implant Placement: British Dental Journal September 2006Louis HutahaeanÎncă nu există evaluări
- Recent Criterias of Tooth Preparation inDocument6 paginiRecent Criterias of Tooth Preparation inFelyciaÎncă nu există evaluări
- Post Insertion Complaints of Removable Dental Prostheses: Original ArticleDocument4 paginiPost Insertion Complaints of Removable Dental Prostheses: Original ArticleAhmed KnaniÎncă nu există evaluări
- Published Immediate ImplantDocument6 paginiPublished Immediate Implantshayma rafatÎncă nu există evaluări
- Dental Implant MaintenanceDocument7 paginiDental Implant MaintenanceLalaÎncă nu există evaluări
- Mouth Preparation For Removable Partial DentureDocument84 paginiMouth Preparation For Removable Partial DentureDrVarun Menon100% (2)
- Endodontic Update 2006Document21 paginiEndodontic Update 2006James LinÎncă nu există evaluări
- Mantenimiento de Prótesis Maxilares ImplantosoportadasDocument10 paginiMantenimiento de Prótesis Maxilares ImplantosoportadasKAREN DANA KARELYA SIQUERO VERAÎncă nu există evaluări
- First Page PDFDocument1 paginăFirst Page PDFhelenbrenda78Încă nu există evaluări
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocument7 paginiThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin SapriÎncă nu există evaluări
- Colleagues For Excellence: Its Role in Retaining Our Patients' Natural DentitionDocument8 paginiColleagues For Excellence: Its Role in Retaining Our Patients' Natural DentitionJessica AnggonoÎncă nu există evaluări
- The Risk of Healing Complications in Primary Teeth With Root FracturesDocument7 paginiThe Risk of Healing Complications in Primary Teeth With Root FracturesRazvan UngureanuÎncă nu există evaluări
- MTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Document6 paginiMTA Pulpotomy As An Alternative To Root Canal Treatment in Children's Permanent Teeth in A Dental Public Health Setting.Abdul Rahman AlmishhdanyÎncă nu există evaluări
- Tips On Implants Vs Endodontically Treated TeethDocument2 paginiTips On Implants Vs Endodontically Treated Teethmarwa2alzemeiÎncă nu există evaluări
- Implant DentistryDocument196 paginiImplant DentistryAkanksha MahajanÎncă nu există evaluări
- Extraction DefectDocument11 paginiExtraction Defectshinomei100% (1)
- Miniscrew-Supported Pole Technique: Surgical-Orthodontic Approach For Impacted or Retained Second Molars in AdolescentsDocument12 paginiMiniscrew-Supported Pole Technique: Surgical-Orthodontic Approach For Impacted or Retained Second Molars in AdolescentsDominikaSkórkaÎncă nu există evaluări
- A Technique For Relining Transitional Removable Denture - A Case ReportDocument4 paginiA Technique For Relining Transitional Removable Denture - A Case ReportEduard Gabriel GavrilăÎncă nu există evaluări
- Practice: Surgical Guidelines For Dental Implant PlacementDocument14 paginiPractice: Surgical Guidelines For Dental Implant PlacementAna94Încă nu există evaluări
- A Guide To Implant Dentistry Part 2 Surgical and Prosthodontic ConsiderationsDocument7 paginiA Guide To Implant Dentistry Part 2 Surgical and Prosthodontic ConsiderationsPhú VinhÎncă nu există evaluări
- Implant ResearchDocument8 paginiImplant ResearchFBI LUC1FeRÎncă nu există evaluări
- Case Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisDocument5 paginiCase Report Massive Radicular Cyst in The Maxillary Sinus As A Result of Deciduous Molar Tooth Pulp NecrosisSarah Ariefah SantriÎncă nu există evaluări
- Risk Management in Clinical Practice. Part 9. Dental ImplantsDocument8 paginiRisk Management in Clinical Practice. Part 9. Dental ImplantsMostafa FayadÎncă nu există evaluări
- Interrelationship Between Periodontics and Restorative DentistryDocument19 paginiInterrelationship Between Periodontics and Restorative DentistrySuperna TiwariÎncă nu există evaluări
- 1 s2.0 S277255962200013X MainDocument10 pagini1 s2.0 S277255962200013X Mainwaf51Încă nu există evaluări
- Immediate Dental ImplantsDocument13 paginiImmediate Dental ImplantsDevanyNataniaÎncă nu există evaluări
- CG A013 04 Stainless Steel Crowns in Deciduous MolarsDocument5 paginiCG A013 04 Stainless Steel Crowns in Deciduous MolarsmahmoudÎncă nu există evaluări
- Use of Non-Vital Pulp Therapies in Primary TeethDocument13 paginiUse of Non-Vital Pulp Therapies in Primary TeethLulamonÎncă nu există evaluări
- Failed Root Canals The Case For Extraction and Immediate Implant PlacementDocument3 paginiFailed Root Canals The Case For Extraction and Immediate Implant PlacementKarin Noga VerhagenÎncă nu există evaluări
- Guidelines For Prescribing Radiographs. Neill SermanDocument7 paginiGuidelines For Prescribing Radiographs. Neill Sermandddemourita9249Încă nu există evaluări
- Treatment Planning Single Maxillary Anterior Implants for DentistsDe la EverandTreatment Planning Single Maxillary Anterior Implants for DentistsÎncă nu există evaluări
- Esthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsDe la EverandEsthetic Oral Rehabilitation with Veneers: A Guide to Treatment Preparation and Clinical ConceptsRichard D. TrushkowskyÎncă nu există evaluări
- Graftless Solutions for the Edentulous PatientDe la EverandGraftless Solutions for the Edentulous PatientSaj JivrajÎncă nu există evaluări
- Abortion and Post Traumatic Stress Disorder - TheresaDocument5 paginiAbortion and Post Traumatic Stress Disorder - TheresaPooja AcharyaÎncă nu există evaluări
- Pcos GuideDocument11 paginiPcos GuidePooja AcharyaÎncă nu există evaluări
- Trismus Aetiology Differentialdiagnosisandtreatment99616Document5 paginiTrismus Aetiology Differentialdiagnosisandtreatment99616Ellizabeth LilantiÎncă nu există evaluări
- Trismus Aetiology Differentialdiagnosisandtreatment99616Document5 paginiTrismus Aetiology Differentialdiagnosisandtreatment99616Ellizabeth LilantiÎncă nu există evaluări
- Neuropsychopharmacology The Fifth Generation of Progress: 5th EditionDocument2.054 paginiNeuropsychopharmacology The Fifth Generation of Progress: 5th EditiondanilomarandolaÎncă nu există evaluări
- DOD MPL Orthodontics Generated From CCQAS For AFMS Use Apr 2014Document2 paginiDOD MPL Orthodontics Generated From CCQAS For AFMS Use Apr 2014aisconsultancy aeÎncă nu există evaluări
- Doctor Mahavir EnclaveDocument22 paginiDoctor Mahavir EnclaveFortune BuildersÎncă nu există evaluări
- Pdhpe Notes FullDocument79 paginiPdhpe Notes FullFarhad HakimiÎncă nu există evaluări
- Nhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaDocument1 paginăNhs Covid Pass - Vaccinated: Covid-19 Vaccine Astrazeneca Covid-19 Vaccine AstrazenecaSuzanne MurphyÎncă nu există evaluări
- Benefits at A Glance: TexasDocument10 paginiBenefits at A Glance: Texasakula_rupeshÎncă nu există evaluări
- Annotated Bibliograhy: Submitted ToDocument4 paginiAnnotated Bibliograhy: Submitted ToRumela Ganguly ChakrabortyÎncă nu există evaluări
- Health Promotion PaperDocument5 paginiHealth Promotion Paperapi-433880230Încă nu există evaluări
- Algemene Huishoudelike Peiling 2018Document203 paginiAlgemene Huishoudelike Peiling 2018Hanlie StadlerÎncă nu există evaluări
- Eligibility List of Faculty Group A Post.Document6 paginiEligibility List of Faculty Group A Post.Stephen HawkingÎncă nu există evaluări
- Sederer Expert Report Publicly FiledDocument157 paginiSederer Expert Report Publicly FiledBrit StackÎncă nu există evaluări
- William Obstetric 24th Study GuideDocument447 paginiWilliam Obstetric 24th Study GuideNizam Kunong100% (2)
- CHED MEMORANDUM ORDER (CMO) No. 14 Series of 2009Document129 paginiCHED MEMORANDUM ORDER (CMO) No. 14 Series of 2009lylesantos85% (48)
- Bahasa Inggris Job InterviewDocument5 paginiBahasa Inggris Job InterviewRahayukurniaÎncă nu există evaluări
- LdavidsonresumeDocument4 paginiLdavidsonresumeapi-270901138Încă nu există evaluări
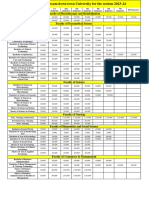
- Fees Structure Assam Down Town University For The Session 2023 2Document2 paginiFees Structure Assam Down Town University For The Session 2023 2Debashish SharmaÎncă nu există evaluări
- Nursing Care (Bing 1)Document6 paginiNursing Care (Bing 1)Shafira ChusnaÎncă nu există evaluări
- Adverse Effects of DrugDocument20 paginiAdverse Effects of DrugABARNA ABIÎncă nu există evaluări
- Case Study Format: (Explain The Aim of The Procedure and Discuss The Significance of The Results, Give Interpretations)Document21 paginiCase Study Format: (Explain The Aim of The Procedure and Discuss The Significance of The Results, Give Interpretations)Maria Teresa Casili - PerezÎncă nu există evaluări
- Treatment of Rheumatoid ArthritisDocument8 paginiTreatment of Rheumatoid Arthritissufian JaganyÎncă nu există evaluări
- Why Your Teamstepps Program May Not Be Working: Timothy C. Clapper, PHD, Grace M. NG, MS, RN, CNM, C-EfmDocument6 paginiWhy Your Teamstepps Program May Not Be Working: Timothy C. Clapper, PHD, Grace M. NG, MS, RN, CNM, C-EfmimÎncă nu există evaluări
- Il.#ji - Ffi: in ofDocument18 paginiIl.#ji - Ffi: in ofMinerva Medical Treatment Pvt LtdÎncă nu există evaluări
- Ra 24Document5 paginiRa 24PhilcarljanAdallaÎncă nu există evaluări
- QB For Mock Test JurisprudenceDocument4 paginiQB For Mock Test JurisprudencePurvak MahajanÎncă nu există evaluări
- 1-N 289 Psychosocial Nursing Overview PPT - Copy-2Document14 pagini1-N 289 Psychosocial Nursing Overview PPT - Copy-2jaÎncă nu există evaluări
- The Singaporean Health Care SystemDocument16 paginiThe Singaporean Health Care SystemKholishotun NufusÎncă nu există evaluări
- Public Health Nurse PHN Final Exam Past Questions For WAHEBDocument3 paginiPublic Health Nurse PHN Final Exam Past Questions For WAHEBCharles Obaleagbon86% (7)
- Social Determinants of Health (SDoH) : Togo, AfricaDocument11 paginiSocial Determinants of Health (SDoH) : Togo, AfricaChantal SpendiffÎncă nu există evaluări
- MPT Musculoskeletal Physiotherapy-Smt Kashibai Navale College of Physiotherapy, Pune - Admission-Details - 20230925204502Document3 paginiMPT Musculoskeletal Physiotherapy-Smt Kashibai Navale College of Physiotherapy, Pune - Admission-Details - 20230925204502hindjai66Încă nu există evaluări
- Freud Background and Test QuestionsDocument4 paginiFreud Background and Test QuestionsLea Amor MerzaÎncă nu există evaluări