S-ar putea să vă placă și
- Collection of MUET Speaking Topics 2020-2023Document89 paginiCollection of MUET Speaking Topics 2020-2023Cikgu Jessie U. Uchat100% (9)
- Medical CertificateDocument2 paginiMedical Certificategcrajasekaran82% (11)
- Method Statement - Fire Rated Duct Insulation.Document16 paginiMethod Statement - Fire Rated Duct Insulation.suhail kalody100% (2)
- Rusty Moore - Visual Impact Cardio PDF-Book Truth & FactsDocument33 paginiRusty Moore - Visual Impact Cardio PDF-Book Truth & FactsNatashaIwashkiw100% (2)
- Essential medicines certificateDocument2 paginiEssential medicines certificateAnji KaringuÎncă nu există evaluări
- InPatient Claim Form - Jubilee Life InsuranceDocument2 paginiInPatient Claim Form - Jubilee Life InsuranceJawad MuhammadÎncă nu există evaluări
- Certificate ADocument4 paginiCertificate ASaurabh MehtaÎncă nu există evaluări
- Medical Claim FormDocument3 paginiMedical Claim Formysraog5@yahoo.comÎncă nu există evaluări
- CSC FORM 41 Med.Document5 paginiCSC FORM 41 Med.editha salahayÎncă nu există evaluări
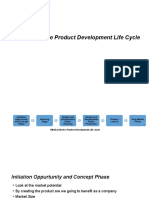
- Medical Device Product Development Life CycleDocument8 paginiMedical Device Product Development Life CycleSuresh Anand100% (1)
- Medical Claim Form B (For Admitted Patient) PDFDocument1 paginăMedical Claim Form B (For Admitted Patient) PDFRakesh rockstarÎncă nu există evaluări
- Hospital Treatment CertificateDocument2 paginiHospital Treatment Certificateayodhya prasad BaghelÎncă nu există evaluări
- Oct 15, 2012 - INDIA (SUN) - This Is The List of 108 of The Most Important Slokas FromDocument26 paginiOct 15, 2012 - INDIA (SUN) - This Is The List of 108 of The Most Important Slokas FromVrajraj DasÎncă nu există evaluări
- Self Attested Proforma For ChildrenDocument1 paginăSelf Attested Proforma For ChildrenBarun Kumar SinghÎncă nu există evaluări
- 5976df9ea1fa813 5190126793 PDFDocument1 pagină5976df9ea1fa813 5190126793 PDFPsycho SoldierÎncă nu există evaluări
- 01.vairagya Triveni - Bhartrihari Vairagya Shatak (Abhilash Saheb, Kabir Ashram, Allahabad)Document110 pagini01.vairagya Triveni - Bhartrihari Vairagya Shatak (Abhilash Saheb, Kabir Ashram, Allahabad)Manohar GathibandheÎncă nu există evaluări
- Medical CertificateDocument1 paginăMedical CertificateArgie Joy Marie AmpolÎncă nu există evaluări
- Medical Certificate Template 12Document1 paginăMedical Certificate Template 12K.O.R. Gaming100% (1)
- Fit PDFDocument1 paginăFit PDFRohith HondazÎncă nu există evaluări
- Medical Leave CertificateDocument1 paginăMedical Leave Certificatenetcity143Încă nu există evaluări
- Hastamalaka Stotram Update Corrections 26may20Document10 paginiHastamalaka Stotram Update Corrections 26may20Alka Bhardwaj100% (1)
- Character investigation questionnaireDocument1 paginăCharacter investigation questionnairetoffee capituloÎncă nu există evaluări
- Gita Commentary TitleDocument820 paginiGita Commentary TitleJuan Pibote100% (1)
- Reporting Suspected Adverse Drug ReactionsDocument2 paginiReporting Suspected Adverse Drug ReactionsRaúl Haimerich MoncadaÎncă nu există evaluări
- Introduction To Vihangam YogaDocument24 paginiIntroduction To Vihangam Yogamahendrachjoshi100% (1)
- Medical Claim B CertificateDocument2 paginiMedical Claim B Certificateanon_712249680Încă nu există evaluări
- Form of Essentiality Certificate BDocument2 paginiForm of Essentiality Certificate BSantosh Kori50% (2)
- Certificate-B MedicalDocument2 paginiCertificate-B MedicalNand Kishore MajhiÎncă nu există evaluări
- Proforma For Claiming Refund of Medical Expenses - 1 - Split - 2Document2 paginiProforma For Claiming Refund of Medical Expenses - 1 - Split - 2ajayÎncă nu există evaluări
- C E R T I F I C A T E - B' To Be Completed in The Case of Patients Who Are Admitted To Hospital For TreatmentDocument2 paginiC E R T I F I C A T E - B' To Be Completed in The Case of Patients Who Are Admitted To Hospital For Treatmentelmore kakaÎncă nu există evaluări
- MergeDocument5 paginiMergeajayÎncă nu există evaluări
- Form of Medical Reimursement ClaimDocument6 paginiForm of Medical Reimursement ClaimViJaY HaLdErÎncă nu există evaluări
- Bsnlmrs FormsDocument5 paginiBsnlmrs FormsdurgendraÎncă nu există evaluări
- Hospitalization Certificate BSNL EmployeeDocument1 paginăHospitalization Certificate BSNL EmployeepradipkshetriÎncă nu există evaluări
- Medical Essential CertificateDocument2 paginiMedical Essential Certificateapi-216708592Încă nu există evaluări
- Medical refund application formDocument5 paginiMedical refund application formAjay SinglaÎncă nu există evaluări
- Medical Certificate More LinesDocument1 paginăMedical Certificate More LinesHuggy MuggyÎncă nu există evaluări
- Medical certificate formDocument1 paginăMedical certificate formShiela Marie Trono-Baral100% (1)
- TPC Medical Claim FormDocument6 paginiTPC Medical Claim FormpenusilaÎncă nu există evaluări
- Certificate: (To Be Filled by The Hospital/ Nursing Home/ Clinic Authority)Document1 paginăCertificate: (To Be Filled by The Hospital/ Nursing Home/ Clinic Authority)Darbha ShaliniÎncă nu există evaluări
- Reimbursement ProformaDocument6 paginiReimbursement ProformaMahesh DewaniÎncă nu există evaluări
- Philippine Civil Service Medical FormDocument1 paginăPhilippine Civil Service Medical FormMica AlcazarÎncă nu există evaluări
- 1582808855278-Reimbursement FormDocument14 pagini1582808855278-Reimbursement FormSuresh MeenaÎncă nu există evaluări
- Claims Form For New India AssuranceDocument2 paginiClaims Form For New India AssuranceRafael BlackÎncă nu există evaluări
- InPatient Claim Form - Jubilee Life InsuranceDocument2 paginiInPatient Claim Form - Jubilee Life InsuranceAhmad Zubair40% (5)
- Heritage Health - Pre Auth FormDocument6 paginiHeritage Health - Pre Auth FormBOOKREADER_NOWÎncă nu există evaluări
- WAPDA Medical Reimbursement FormDocument1 paginăWAPDA Medical Reimbursement FormMirza Sohail Ahmad SoharwardiÎncă nu există evaluări
- Affidavit No Professional Fee ChargedDocument1 paginăAffidavit No Professional Fee ChargedReegan MasarateÎncă nu există evaluări
- Cancer Patient Airfare Concession FormDocument1 paginăCancer Patient Airfare Concession Formkrishnadas nairÎncă nu există evaluări
- Notification of Claim - Prudential GuaranteeDocument2 paginiNotification of Claim - Prudential GuaranteeZen Catolico ErumÎncă nu există evaluări
- Medical Certificate (Form 41)Document1 paginăMedical Certificate (Form 41)Nasra AbdulganiÎncă nu există evaluări
- Credential IngDocument13 paginiCredential Ingdr_rajatjainÎncă nu există evaluări
- Medical Claim Form (Reimbursement Only)Document2 paginiMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- CS Form 41 medical certificateDocument1 paginăCS Form 41 medical certificateLucenda CabayloÎncă nu există evaluări
- Medical Leave Fitness Certificatepdf Commutation of Leave Medical Certificate For Leave or Circ OrgDocument1 paginăMedical Leave Fitness Certificatepdf Commutation of Leave Medical Certificate For Leave or Circ OrgKrishna PrasadÎncă nu există evaluări
- In-Patient Claim FormDocument2 paginiIn-Patient Claim Formfaisal_1241Încă nu există evaluări
- Medical Reimbursement FormDocument2 paginiMedical Reimbursement FormMEMOONA ASHARÎncă nu există evaluări
- DepEd Medical CertificateDocument1 paginăDepEd Medical CertificateMaria Eleonor C. BañaresÎncă nu există evaluări
- ChecklistDocument9 paginiChecklistkarthikfuser0183Încă nu există evaluări
- Application Med. Re-ImbDocument2 paginiApplication Med. Re-Imbzahid hussainÎncă nu există evaluări
- medical formDocument3 paginimedical formTahir HussainÎncă nu există evaluări
- PhilHealth Hospital Accreditation ChecklistDocument14 paginiPhilHealth Hospital Accreditation Checklistamira_hassan100% (1)
- Medical Form, Outdoor Certificate - ADocument2 paginiMedical Form, Outdoor Certificate - Anaresh yadavÎncă nu există evaluări
- Medical Claims Form ExplainedDocument4 paginiMedical Claims Form ExplainedShibayan SarkarÎncă nu există evaluări
- Bài tập Prefixes và các trường hợp nghiên cứu gãy xương đùiDocument3 paginiBài tập Prefixes và các trường hợp nghiên cứu gãy xương đùiNgoc SherlockÎncă nu există evaluări
- SolAcne - A Manufacturer of Dermatological Cosmetics Releases Full Anti-Acne Protection Set in EuropeDocument2 paginiSolAcne - A Manufacturer of Dermatological Cosmetics Releases Full Anti-Acne Protection Set in EuropePR.comÎncă nu există evaluări
- Webinar - I-WPS OfficeDocument31 paginiWebinar - I-WPS OfficeGayathri sundarajanÎncă nu există evaluări
- Establishing VAW Desk GuidelinesDocument3 paginiEstablishing VAW Desk Guidelinesjudith buenoÎncă nu există evaluări
- Assessment of Haematological Parameter and Liver Enzyme Among Hepatitis B Infected Blood DonorsDocument9 paginiAssessment of Haematological Parameter and Liver Enzyme Among Hepatitis B Infected Blood DonorsKIU PUBLICATION AND EXTENSIONÎncă nu există evaluări
- Biology: Cambridge International Examinations International General Certificate of Secondary EducationDocument20 paginiBiology: Cambridge International Examinations International General Certificate of Secondary Educationmath magicÎncă nu există evaluări
- Pharma - M6L2 - Drug Therapy For OA and Gouty ArthritisDocument8 paginiPharma - M6L2 - Drug Therapy For OA and Gouty ArthritisAngelaTrinidadÎncă nu există evaluări
- Final Rationale CVDocument86 paginiFinal Rationale CVFaith Renzel RoxasÎncă nu există evaluări
- 19th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation AssociationDocument3 pagini19th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation AssociationNia Kania HapsyahÎncă nu există evaluări
- Course Code Description Units Pre-Requisite: Obe CurriculumDocument2 paginiCourse Code Description Units Pre-Requisite: Obe CurriculumShyla ManguiatÎncă nu există evaluări
- Model Factories Rules As On 01.03.2019Document257 paginiModel Factories Rules As On 01.03.2019Latest Laws TeamÎncă nu există evaluări
- Codythomas MethodsmatrixDocument8 paginiCodythomas Methodsmatrixapi-563955428Încă nu există evaluări
- Calculating Pediatric Medication and Fluid DosagesDocument5 paginiCalculating Pediatric Medication and Fluid DosagesMayank KumarÎncă nu există evaluări
- 02 - February RsmiDocument123 pagini02 - February RsmiAlex SibalÎncă nu există evaluări
- Standard Operating Procedure: Scope / PurposeDocument2 paginiStandard Operating Procedure: Scope / PurposeAdrian RuizÎncă nu există evaluări
- KesdjianaDocument5 paginiKesdjianaKonstantinos CharalampousÎncă nu există evaluări
- Market Research TRAIN LAWDocument60 paginiMarket Research TRAIN LAWRusselÎncă nu există evaluări
- Endeavour - 01x03 - Rocket - fov.English.C.updated - SujaidrDocument100 paginiEndeavour - 01x03 - Rocket - fov.English.C.updated - SujaidrRarities edicionesÎncă nu există evaluări
- Aetna Student Health pre-determination requestDocument3 paginiAetna Student Health pre-determination requestUmi KhanÎncă nu există evaluări
- Ergonomic 2Document45 paginiErgonomic 2Akhilesh Kumar SinghÎncă nu există evaluări
- Academic stress and exam anxiety among Indian secondary studentsDocument19 paginiAcademic stress and exam anxiety among Indian secondary studentsAnonymous Is3m4q2JqWÎncă nu există evaluări
- Reaction Paper On Son RiseDocument3 paginiReaction Paper On Son RiseCarlo P. Carlon71% (14)
- PPE Toolbox TalkDocument2 paginiPPE Toolbox TalkSubhi El Haj SalehÎncă nu există evaluări
- Chapter 5 ENGLISHDocument24 paginiChapter 5 ENGLISHvenda novi riantaÎncă nu există evaluări
- Template School ProfileDocument4 paginiTemplate School ProfileCaitlin PeñeraÎncă nu există evaluări
- Yacon Syrup: Principles and ProcessingDocument40 paginiYacon Syrup: Principles and Processingstephen puleiÎncă nu există evaluări