S-ar putea să vă placă și
- Drugs Used in Liver DiseaseDocument17 paginiDrugs Used in Liver Diseaseblast2111Încă nu există evaluări
- Rotation PlanDocument1 paginăRotation Planblast2111Încă nu există evaluări
- Neonatal Resuscitation DrugsDocument4 paginiNeonatal Resuscitation Drugsblast2111Încă nu există evaluări
- Family AssessmentDocument13 paginiFamily Assessmentblast211140% (5)
- Tracheo Esophageal FistulaDocument6 paginiTracheo Esophageal Fistulablast2111Încă nu există evaluări
- Group DynamicsDocument12 paginiGroup Dynamicsblast2111100% (1)
- Essential Newborn CareDocument8 paginiEssential Newborn Careblast2111Încă nu există evaluări
- Programmed InstructionDocument7 paginiProgrammed Instructionblast2111Încă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Anterior RhinosDocument4 paginiAnterior RhinosYohan YudhantoÎncă nu există evaluări
- MUL, Dick PDFDocument240 paginiMUL, Dick PDFNursyamsuddin MoganaÎncă nu există evaluări
- Tetany in Hand-Reared Common Brushtail Possums: DR Jim Pollock B.V.SC Wildlife VeterinarianDocument21 paginiTetany in Hand-Reared Common Brushtail Possums: DR Jim Pollock B.V.SC Wildlife VeterinarianPossum TVÎncă nu există evaluări
- Sufixe Si PrefixeDocument14 paginiSufixe Si Prefixeseaofdreams6Încă nu există evaluări
- Erotic Sms Page 1Document12 paginiErotic Sms Page 1Ashish AroraÎncă nu există evaluări
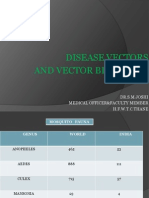
- Disease Vectors and Vector BionomicsDocument16 paginiDisease Vectors and Vector BionomicsSuhas JoshiÎncă nu există evaluări
- Diagnosis, Parasitose em AvesDocument10 paginiDiagnosis, Parasitose em AvesRoberio OlindaÎncă nu există evaluări
- B CellDocument10 paginiB CellSonia Elizabeth SimonÎncă nu există evaluări
- 0610 m16 Ms 42Document10 pagini0610 m16 Ms 42Keshav JindalÎncă nu există evaluări
- Jump To Navigation Jump To Search: For Other Uses, SeeDocument19 paginiJump To Navigation Jump To Search: For Other Uses, SeeDanny FentomÎncă nu există evaluări
- Current Clinical Concepts in Regenerative Periodontal Therapy PDFDocument8 paginiCurrent Clinical Concepts in Regenerative Periodontal Therapy PDFFergy Christin MaitimuÎncă nu există evaluări
- MER 2.0.0 Indicator Reference GuideDocument174 paginiMER 2.0.0 Indicator Reference GuideMigori Art DataÎncă nu există evaluări
- Whales Dolphins Gulf of Mexico PosterDocument1 paginăWhales Dolphins Gulf of Mexico PosterPaleogeneÎncă nu există evaluări
- NCP-Ineffective Airway ClearanceDocument13 paginiNCP-Ineffective Airway ClearancePaulo Manlangit86% (22)
- Jose P. Laurel Sr. High SchoolDocument8 paginiJose P. Laurel Sr. High SchoolEricha SolomonÎncă nu există evaluări
- Postnatal Growth and Development: Yenny Yustisia Dept. of Oral Biology Dentistry UNEJDocument38 paginiPostnatal Growth and Development: Yenny Yustisia Dept. of Oral Biology Dentistry UNEJMelisa Novitasari100% (1)
- Dopamine&Oxytocin DisordersDocument32 paginiDopamine&Oxytocin Disorderselberto2Încă nu există evaluări
- Food Borne Diseases and Its PreventionDocument181 paginiFood Borne Diseases and Its Preventionapi-19916399Încă nu există evaluări
- Essential Intrapartum and Newborn CareDocument2 paginiEssential Intrapartum and Newborn CareNikka Moreen DagdagÎncă nu există evaluări
- Hotspots Magazine - 2015-09-01Document104 paginiHotspots Magazine - 2015-09-01Holstein PlazaÎncă nu există evaluări
- 5090 s16 Ms 22 PDFDocument10 pagini5090 s16 Ms 22 PDFclydeÎncă nu există evaluări
- Professional Anesthesia HandbookDocument114 paginiProfessional Anesthesia HandbookSooryajith DineshÎncă nu există evaluări
- Physical Form 2018Document2 paginiPhysical Form 2018api-247134277Încă nu există evaluări
- Fats and The BrainDocument8 paginiFats and The BrainRade NovakovicÎncă nu există evaluări
- Journal 1 - Plasenta PreviaDocument5 paginiJournal 1 - Plasenta Previarizky ferdina kevinÎncă nu există evaluări
- DR Deagle's H1N1 ReportDocument61 paginiDR Deagle's H1N1 Reportkingofswords100% (1)
- Trigeminal Nerve: Dr.B.B.GosaiDocument76 paginiTrigeminal Nerve: Dr.B.B.GosaiAlexAlxÎncă nu există evaluări
- Housing Systems of PoultryDocument7 paginiHousing Systems of PoultryferdinandÎncă nu există evaluări
- ErytropoiesisDocument23 paginiErytropoiesiswarda farooqÎncă nu există evaluări
- ThyroidDocument7 paginiThyroidverawoÎncă nu există evaluări