S-ar putea să vă placă și
- ASLIA Code of EthicsDocument9 paginiASLIA Code of Ethicsramtintbkh100% (1)
- Aplicación NAATI para TraductorDocument20 paginiAplicación NAATI para TraductorNatalia100% (1)
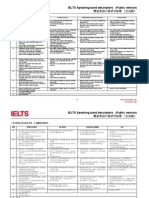
- IELTS Speaking band descriptors explainedDocument2 paginiIELTS Speaking band descriptors explainedclinta1979100% (1)
- Literal Vs Liberal What Is A Faithful inDocument34 paginiLiteral Vs Liberal What Is A Faithful inMisarabbit NguyenÎncă nu există evaluări
- PSPTIS101 Assessment Task WorkbookDocument17 paginiPSPTIS101 Assessment Task WorkbookGRACEÎncă nu există evaluări
- Working with Interpreters in South Australian CourtsDocument20 paginiWorking with Interpreters in South Australian Courtskamal ferozÎncă nu există evaluări
- Coping With Culture in Media InterpretingDocument21 paginiCoping With Culture in Media Interpretinglixiaoxiu100% (3)
- Improvements To NAATI TestingDocument132 paginiImprovements To NAATI TestingMinh Trang NguyễnÎncă nu există evaluări
- PSPTIS002-Building Glossaries For Translating and Interpreting AssignmentsDocument26 paginiPSPTIS002-Building Glossaries For Translating and Interpreting AssignmentsmaggieÎncă nu există evaluări
- Positive Partnerships Planning MatrixDocument17 paginiPositive Partnerships Planning Matrixmelanie-304041Încă nu există evaluări
- NAATIINTERPETER Certification Scheme Design SummaryDocument5 paginiNAATIINTERPETER Certification Scheme Design SummaryYaksá HiperbólicoÎncă nu există evaluări
- Planning Matrix For Assessment 2-2Document3 paginiPlanning Matrix For Assessment 2-2api-299768321Încă nu există evaluări
- Certification Scheme For NAATIDocument5 paginiCertification Scheme For NAATINatalia100% (1)
- Naati Testing Format - Paraprofessional Interpreter: Section One: Cultural and Social Aspects (5 Mins)Document6 paginiNaati Testing Format - Paraprofessional Interpreter: Section One: Cultural and Social Aspects (5 Mins)Arijit Das AvroÎncă nu există evaluări
- A Textbook of InterpretingDocument72 paginiA Textbook of InterpretingKatia KatiaÎncă nu există evaluări
- The Sign Language InterpretedDocument13 paginiThe Sign Language InterpretedBecky SkolnickÎncă nu există evaluări
- Breaking the Sound Barriers: 9 deaf success storiesDe la EverandBreaking the Sound Barriers: 9 deaf success storiesEvaluare: 4.5 din 5 stele4.5/5 (3)
- Approaches To Social ResearchDocument209 paginiApproaches To Social ResearchRocío ZubillagaÎncă nu există evaluări
- Introduction To NAATI CCL Urdu TestDocument29 paginiIntroduction To NAATI CCL Urdu TestSajjad Rasool ChaudhryÎncă nu există evaluări
- s3 - Differentiated Learning ExperienceDocument7 paginis3 - Differentiated Learning Experienceapi-478887066Încă nu există evaluări
- Sign Language of the North American Indians (Illustrated Edition): Compared With That Among Other Peoples And Deaf-MutesDe la EverandSign Language of the North American Indians (Illustrated Edition): Compared With That Among Other Peoples And Deaf-MutesÎncă nu există evaluări
- Transforming TraditionDocument17 paginiTransforming TraditionRangga LailÎncă nu există evaluări
- Deafness, Disability and Inclusion: The Gap Between Rhetoric and PracticeDocument18 paginiDeafness, Disability and Inclusion: The Gap Between Rhetoric and PracticelitsakipÎncă nu există evaluări
- IFLA Library Building Guidelines - Development and ReflectionDocument305 paginiIFLA Library Building Guidelines - Development and Reflectiondede100% (1)
- DST 710-Hy01 Syllabus Summer 2017Document10 paginiDST 710-Hy01 Syllabus Summer 2017api-319843117Încă nu există evaluări
- Hedgerow-Survey-Handbook 2nd Ed (DEFRA)Document143 paginiHedgerow-Survey-Handbook 2nd Ed (DEFRA)Chromaticghost2Încă nu există evaluări
- Errors, Omissions and Infelicities in Broadcast InterpretingDocument20 paginiErrors, Omissions and Infelicities in Broadcast InterpretingDario Matteo Sparanero100% (1)
- EDC GuidanceDocument36 paginiEDC GuidanceferasallanÎncă nu există evaluări
- Guideline for Hearing Aid Fitting in Children and AdultsDocument80 paginiGuideline for Hearing Aid Fitting in Children and AdultsPhillip Martinez50% (2)
- BMDC Telemedicine Guidelines July2020Document41 paginiBMDC Telemedicine Guidelines July2020Mensa DigiWorldÎncă nu există evaluări
- Tikanga A Rongoa Apr14 v2Document53 paginiTikanga A Rongoa Apr14 v2Vivian Hurtado AhumadaÎncă nu există evaluări
- SAQ123 NursesUserGuide V6Document30 paginiSAQ123 NursesUserGuide V6LisaBrook100% (1)
- Uq727331 OaDocument15 paginiUq727331 OatwinforsyriaÎncă nu există evaluări
- Oral Health ProgramDocument8 paginiOral Health Programapi-292263050Încă nu există evaluări
- Equal Access To Healthcare: The Importance of Accessible Healthcare Services For People Who Are DeafblindDocument38 paginiEqual Access To Healthcare: The Importance of Accessible Healthcare Services For People Who Are DeafblindErn NievaÎncă nu există evaluări
- Standards for Primary Care FacilitiesDocument52 paginiStandards for Primary Care FacilitiesJason Suquila100% (1)
- Public Health Directorate ConsultantDocument17 paginiPublic Health Directorate Consultantcristinusc@gmail.comÎncă nu există evaluări
- Case Study 1 Riverland General Hospital and Country Health SaDocument7 paginiCase Study 1 Riverland General Hospital and Country Health SaFaheem YaseenÎncă nu există evaluări
- PD2014 028Document30 paginiPD2014 028Inne Milagros FransienDimpudusÎncă nu există evaluări
- Health in Practice ProgrammeDocument6 paginiHealth in Practice Programmeevan mannionÎncă nu există evaluări
- Drug Prescribing For DentistsDocument84 paginiDrug Prescribing For Dentistsmoheen_khanÎncă nu există evaluări
- Drugs 3Document43 paginiDrugs 3IonuțHerpeșÎncă nu există evaluări
- The Cost of CareDocument3 paginiThe Cost of CareSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Palliative Care Guidelines-20 November2013Document69 paginiPalliative Care Guidelines-20 November2013Olga ŢiuÎncă nu există evaluări
- Public Health Assistant - Generic JD 0Document8 paginiPublic Health Assistant - Generic JD 0Mahamoud Suleiman MohamedÎncă nu există evaluări
- P TeledentistryDocument3 paginiP Teledentistrypooja singhÎncă nu există evaluări
- Rujukan OrtoDocument8 paginiRujukan OrtoJade M. LolongÎncă nu există evaluări
- FPCSM 2014 PDFDocument441 paginiFPCSM 2014 PDFRyan Michael OducadoÎncă nu există evaluări
- 1.national Guide To A Preventive Health Assessment For Aboriginal and Torres Strait Islander PeopleDocument100 pagini1.national Guide To A Preventive Health Assessment For Aboriginal and Torres Strait Islander PeopleRumana AliÎncă nu există evaluări
- Emergency Medicine Locum AppointmentDocument13 paginiEmergency Medicine Locum AppointmentQusaiBadrÎncă nu există evaluări
- Seba Saqer - 20180482 Puplic HealthDocument9 paginiSeba Saqer - 20180482 Puplic HealthSaba SaqerÎncă nu există evaluări
- Public vs Private DentistryDocument18 paginiPublic vs Private DentistrySaba SaqerÎncă nu există evaluări
- Operational Guidelines Ear, Nose and Throat (ENT) Care at HWCsDocument32 paginiOperational Guidelines Ear, Nose and Throat (ENT) Care at HWCsAnagha M NairÎncă nu există evaluări
- NATIONAL GUIDELINES FOR PX and MX OF RTISTD PDFDocument105 paginiNATIONAL GUIDELINES FOR PX and MX OF RTISTD PDFhemihemaÎncă nu există evaluări
- National Guidelines For The Use of Complementary Therapies in Supportive and Palliative CareDocument112 paginiNational Guidelines For The Use of Complementary Therapies in Supportive and Palliative Caredorothywyn50% (2)
- SoPs Dental Assistants and Dental Hygienist For PublicationDocument10 paginiSoPs Dental Assistants and Dental Hygienist For PublicationFawad AhmadÎncă nu există evaluări
- Terms of Reference Physician SpecialistDocument6 paginiTerms of Reference Physician Specialistgk983195Încă nu există evaluări
- DH Notes - Dental Hygienist's Chairside Pocket GuideDocument231 paginiDH Notes - Dental Hygienist's Chairside Pocket GuideHany L Hossainy100% (4)
- Walhalla Gold MineDocument1 paginăWalhalla Gold MineYwagar YwagarÎncă nu există evaluări
- Sydney 2008 MarchDocument8 paginiSydney 2008 MarchYwagar YwagarÎncă nu există evaluări
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDocument14 paginiClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarÎncă nu există evaluări
- AMC Clinical Exam Recall 8 Sep 2008 Melbourne Retest 1Document7 paginiAMC Clinical Exam Recall 8 Sep 2008 Melbourne Retest 1Ywagar YwagarÎncă nu există evaluări
- Adelaide, 5 April, 2008: PaediatricsDocument17 paginiAdelaide, 5 April, 2008: PaediatricsYwagar YwagarÎncă nu există evaluări
- Recall Brisbane February 2008Document7 paginiRecall Brisbane February 2008Ywagar YwagarÎncă nu există evaluări
- GPDocument3 paginiGPYwagar YwagarÎncă nu există evaluări
- Brisbane July 2008 RecallDocument11 paginiBrisbane July 2008 RecallYwagar YwagarÎncă nu există evaluări
- Gold Coast 2008Document1 paginăGold Coast 2008Ywagar YwagarÎncă nu există evaluări
- Draft May 08 WES ProgramDocument2 paginiDraft May 08 WES ProgramYwagar YwagarÎncă nu există evaluări
- Dr CAI clinical cases under 40 charsDocument31 paginiDr CAI clinical cases under 40 charsYwagar Ywagar100% (1)
- Adelaide April 2008Document16 paginiAdelaide April 2008Ywagar YwagarÎncă nu există evaluări
- Melbourne 2008 Nov 8Document10 paginiMelbourne 2008 Nov 8Ywagar YwagarÎncă nu există evaluări
- Adelaide 13th September 2008Document16 paginiAdelaide 13th September 2008Ywagar YwagarÎncă nu există evaluări
- Adelaide 13th September 2008Document16 paginiAdelaide 13th September 2008Ywagar YwagarÎncă nu există evaluări
- Syd 1Document11 paginiSyd 1Ywagar YwagarÎncă nu există evaluări
- Adel 2Document24 paginiAdel 2Ywagar YwagarÎncă nu există evaluări
- Adelaide 13th September 2008Document16 paginiAdelaide 13th September 2008Ywagar YwagarÎncă nu există evaluări
- Paediatrics:: Case 1nsionDocument16 paginiPaediatrics:: Case 1nsionYwagar YwagarÎncă nu există evaluări
- Melb RetestDocument6 paginiMelb RetestYwagar YwagarÎncă nu există evaluări
- MelbDocument9 paginiMelbYwagar YwagarÎncă nu există evaluări
- ACln2007!09!08MEL Retest Wd97Document6 paginiACln2007!09!08MEL Retest Wd97Ywagar YwagarÎncă nu există evaluări
- Brisbane, 11th October 2008Document6 paginiBrisbane, 11th October 2008Ywagar YwagarÎncă nu există evaluări
- Melb RetestDocument2 paginiMelb RetestYwagar YwagarÎncă nu există evaluări
- To ReviseAug 22 AdelaideDocument4 paginiTo ReviseAug 22 AdelaideYwagar YwagarÎncă nu există evaluări
- BrisDocument9 paginiBrisYwagar YwagarÎncă nu există evaluări
- Brisbane, 11th October 2008Document6 paginiBrisbane, 11th October 2008Ywagar YwagarÎncă nu există evaluări
- Melb RetestDocument4 paginiMelb RetestYwagar YwagarÎncă nu există evaluări
- 9 August 08 Melbourne Clinical Exam RecallDocument6 pagini9 August 08 Melbourne Clinical Exam RecallYwagar YwagarÎncă nu există evaluări
- Clinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeDocument14 paginiClinical Recall 17 May 2008 Melbourne: AMC Feedback: Sudden Infant Death SyndromeYwagar YwagarÎncă nu există evaluări
- Tai Gruver: ASL TeacherDocument4 paginiTai Gruver: ASL Teacherapi-727684075Încă nu există evaluări
- HSG 19 7Document8 paginiHSG 19 7Nguyễn T. KiênÎncă nu există evaluări
- Sign To Letter Translator System Using A Hand Glove: April 2014Document6 paginiSign To Letter Translator System Using A Hand Glove: April 2014Bhupendra(Rahul...) kumarÎncă nu există evaluări
- Euphemism ZJDocument18 paginiEuphemism ZJSihem AbbassiÎncă nu există evaluări
- Hand gesture recognition for communicationDocument55 paginiHand gesture recognition for communicationSaurabh shuklaÎncă nu există evaluări
- Lesson 4 - Types and Level of CommunicationDocument9 paginiLesson 4 - Types and Level of CommunicationMary Rose Bobis VicenteÎncă nu există evaluări
- Machine Translation System for Ethiopian Sign LanguageDocument7 paginiMachine Translation System for Ethiopian Sign Languageashenafi100% (1)
- 23Document13 pagini23yamedagomenasaiÎncă nu există evaluări
- LANGUAGE and WritingDocument39 paginiLANGUAGE and WritingEdu Manzano AlbayÎncă nu există evaluări
- Effective English Teaching: Communication Skills, Language Features & TypesDocument2 paginiEffective English Teaching: Communication Skills, Language Features & TypesGeorgia CassavaÎncă nu există evaluări
- Types of Space and Their Use in Sign LanguageDocument11 paginiTypes of Space and Their Use in Sign LanguageLourenço MoreiraÎncă nu există evaluări
- Cambridge University Press Journal of LinguisticsDocument6 paginiCambridge University Press Journal of LinguisticsPaulo PilarÎncă nu există evaluări
- Applied linguistics explores language issuesDocument5 paginiApplied linguistics explores language issuesJorge zamora.romero RomeroÎncă nu există evaluări
- COLONOMUS 2018 - Deaf-HeartDocument8 paginiCOLONOMUS 2018 - Deaf-HeartKarina Borges LimaÎncă nu există evaluări
- Asl Lesson Plan PDFDocument6 paginiAsl Lesson Plan PDFapi-284961463Încă nu există evaluări
- Dokumen - Pub The Gallaudet Dictionary of American Sign Language 1954622015 9781954622012Document601 paginiDokumen - Pub The Gallaudet Dictionary of American Sign Language 1954622015 9781954622012Livo100% (1)
- Sign Language To Voice ConverterDocument13 paginiSign Language To Voice ConverterAnoop K VenuÎncă nu există evaluări
- Reading 2Document3 paginiReading 2Ninjin NerguidavaaÎncă nu există evaluări
- Let's Check! Sign LanguagesDocument4 paginiLet's Check! Sign LanguagesEdrick ParasÎncă nu există evaluări
- The Valences of Total CommunicationDocument7 paginiThe Valences of Total CommunicationnituvvvÎncă nu există evaluări
- ASL Grammar sw0011 ASL Grammar 01 PDFDocument10 paginiASL Grammar sw0011 ASL Grammar 01 PDFAnderson HenriqueÎncă nu există evaluări
- Bài tập unit 10 anh 8 (P)Document8 paginiBài tập unit 10 anh 8 (P)Trần Thị Kim LiênÎncă nu există evaluări
- Soal Tambahan AlumniDocument3 paginiSoal Tambahan AlumniDeslina Uskharini100% (1)
- Social and individual bilingualism in deaf communitiesDocument8 paginiSocial and individual bilingualism in deaf communitiesFikhy PramudiÎncă nu există evaluări
- ПРОБНИЙ ТЕСТ У ФОРМАТІ ЗОВНІШНЬОГО НЕЗАЛЕЖНОГО ОЦІНЮВАННЯ З АНГЛІЙСЬКОЇDocument15 paginiПРОБНИЙ ТЕСТ У ФОРМАТІ ЗОВНІШНЬОГО НЕЗАЛЕЖНОГО ОЦІНЮВАННЯ З АНГЛІЙСЬКОЇAnastasiia PopovaÎncă nu există evaluări
- The Usage of Language in Enhancing Communication Processes: Dr. Radhika KapurDocument12 paginiThe Usage of Language in Enhancing Communication Processes: Dr. Radhika KapurTalent NzvengaÎncă nu există evaluări
- Hopscotch 6 End-Of-Term 1 Test PDFDocument6 paginiHopscotch 6 End-Of-Term 1 Test PDForadu1395Încă nu există evaluări
- Designing For People With Visual DisabilitiesDocument14 paginiDesigning For People With Visual DisabilitiesBrian ChiefÎncă nu există evaluări
- Sign Language: Presented by 01211805309 Under The Guidance ofDocument29 paginiSign Language: Presented by 01211805309 Under The Guidance ofhrsh_palÎncă nu există evaluări
- Olinco 2013 AbstractsDocument173 paginiOlinco 2013 AbstractsaelyssÎncă nu există evaluări