S-ar putea să vă placă și
- Model InvatareDocument1 paginăModel InvataretraducanÎncă nu există evaluări
- Engleza Cursuri IncepatoriDocument70 paginiEngleza Cursuri IncepatoriSimonca VasileÎncă nu există evaluări
- Manual EnglezaDocument92 paginiManual EnglezaAmalia TatuÎncă nu există evaluări
- Animal LearningDocument292 paginiAnimal LearningtraducanÎncă nu există evaluări
- NC ExitDocument2 paginiNC ExitdinhhaphucÎncă nu există evaluări
- Parole AOEDocument2 paginiParole AOEtraducanÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Plato and The StatesmanDocument18 paginiPlato and The StatesmanTzoutzoukinaÎncă nu există evaluări
- Cooling TowerDocument67 paginiCooling TowerMayank BhardwajÎncă nu există evaluări
- Trends M2Document14 paginiTrends M2BUNTA, NASRAIDAÎncă nu există evaluări
- Lecture 03 PDFDocument13 paginiLecture 03 PDFHemanth KumarÎncă nu există evaluări
- Vidler - Architecture's Expanded FieldDocument8 paginiVidler - Architecture's Expanded FieldNelson Stiven SánchezÎncă nu există evaluări
- Marketing PlanDocument40 paginiMarketing PlanKapeel LeemaniÎncă nu există evaluări
- Factors Influencing Purchase Intention in Online ShoppingDocument14 paginiFactors Influencing Purchase Intention in Online ShoppingSabrina O. SihombingÎncă nu există evaluări
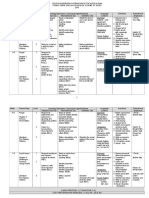
- English Form 3 Scheme of Work 2016Document8 paginiEnglish Form 3 Scheme of Work 2016jayavesovalingamÎncă nu există evaluări
- TKI Conflict Resolution ModelDocument2 paginiTKI Conflict Resolution ModelClerenda McgradyÎncă nu există evaluări
- Introduction To Statistics: There Are Two Major Divisions of Inferential Statistics: Confidence IntervalDocument8 paginiIntroduction To Statistics: There Are Two Major Divisions of Inferential Statistics: Confidence IntervalSadi The-Darkraven KafiÎncă nu există evaluări
- Decode Secret MessageDocument4 paginiDecode Secret MessageChristian BucalÎncă nu există evaluări
- Fiitjee Rmo Mock TestDocument7 paginiFiitjee Rmo Mock TestAshok DargarÎncă nu există evaluări
- Values EducationDocument7 paginiValues EducationgosmileyÎncă nu există evaluări
- A Study On Learning and Competency Development of Employees at SRF LTDDocument4 paginiA Study On Learning and Competency Development of Employees at SRF LTDLakshmiRengarajanÎncă nu există evaluări
- XI & XII Half Yearly Exam (2022 - 2023)Document1 paginăXI & XII Half Yearly Exam (2022 - 2023)Abhinaba BanikÎncă nu există evaluări
- Science Technology and SocietyDocument9 paginiScience Technology and SocietyAries Ganot100% (1)
- Max Stirner, The Lunatic and Donald Trump Michael McAnear, PHD Department of Arts and Humanities National UniversityDocument4 paginiMax Stirner, The Lunatic and Donald Trump Michael McAnear, PHD Department of Arts and Humanities National UniversityLibrairie IneffableÎncă nu există evaluări
- History of Human Resource ManagementDocument19 paginiHistory of Human Resource ManagementNaila MehboobÎncă nu există evaluări
- Non Experimental Research 1Document22 paginiNon Experimental Research 1Daphane Kate AureadaÎncă nu există evaluări
- My Resignation by James HallDocument17 paginiMy Resignation by James HallAustin Macauley Publishers Ltd.Încă nu există evaluări
- Dunton 2019....................................................Document18 paginiDunton 2019....................................................Gayathri manojÎncă nu există evaluări
- Felix Amante Senior High School: Division of San Pablo City San Pablo CityDocument2 paginiFelix Amante Senior High School: Division of San Pablo City San Pablo CityKaye Ann CarelÎncă nu există evaluări
- ART Thesis JozwiakJ 2014Document194 paginiART Thesis JozwiakJ 2014Stuart OringÎncă nu există evaluări
- Proclus On The Theology of Plato, Thomas TaylorDocument593 paginiProclus On The Theology of Plato, Thomas TaylorWaterwind100% (2)
- Four Tendencies QuizDocument5 paginiFour Tendencies Quizsweetambition33% (3)
- Sense of Control Under Uncertainty Depends On People's Childhood Environment: A Life History Theory ApproachDocument17 paginiSense of Control Under Uncertainty Depends On People's Childhood Environment: A Life History Theory ApproachRiazboniÎncă nu există evaluări
- Papademetriou - Performative Meaning of the Word παρρησία in Ancient Greek and in the Greek BibleDocument26 paginiPapademetriou - Performative Meaning of the Word παρρησία in Ancient Greek and in the Greek BibleKernal StefanieÎncă nu există evaluări
- Asset Management ISO55Document50 paginiAsset Management ISO55helix2010Încă nu există evaluări
- Classical and Operant Conditioning: Group 1 Shravan Abraham Ashwini Sindura Sadanandan Sneha JohnDocument15 paginiClassical and Operant Conditioning: Group 1 Shravan Abraham Ashwini Sindura Sadanandan Sneha JohnSindura SadanandanÎncă nu există evaluări
- Hussian Matrix Economic Applications PDFDocument51 paginiHussian Matrix Economic Applications PDFSiddi RamuluÎncă nu există evaluări