S-ar putea să vă placă și
- Roast Chicken With Couscous & Pine Nut StuffingDocument2 paginiRoast Chicken With Couscous & Pine Nut StuffinganonymousÎncă nu există evaluări
- Personality DisordersDocument7 paginiPersonality DisordersanonymousÎncă nu există evaluări
- IV Fluid ChartDocument2 paginiIV Fluid Charthady920Încă nu există evaluări
- Trauma Management NotesDocument5 paginiTrauma Management NotesanonymousÎncă nu există evaluări
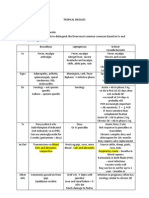
- Tropical DiseasesDocument4 paginiTropical DiseasesanonymousÎncă nu există evaluări
- Diagnostic Imaging For Back Pain AFP 2004Document5 paginiDiagnostic Imaging For Back Pain AFP 2004anonymousÎncă nu există evaluări
- SIDE EFFECTS OCD AntipsychoticsDocument9 paginiSIDE EFFECTS OCD AntipsychoticsanonymousÎncă nu există evaluări
- NIH Stroke Scale Exam Order Form21Document1 paginăNIH Stroke Scale Exam Order Form21anonymousÎncă nu există evaluări
- Medical MnemonicsDocument10 paginiMedical Mnemonicskenners99% (115)
- CPG Clinician Full BipolarDocument26 paginiCPG Clinician Full BipolaranonymousÎncă nu există evaluări
- FRACP Long Case NotesDocument10 paginiFRACP Long Case Notesanonymous0% (1)
- Algorithm - Recognition of Dementia in Hospitalised Older AdultsDocument2 paginiAlgorithm - Recognition of Dementia in Hospitalised Older AdultsanonymousÎncă nu există evaluări
- Outbreak GuidelineDocument20 paginiOutbreak GuidelineanonymousÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Contemporary Leadership Theories and StylesDocument21 paginiContemporary Leadership Theories and StylesBuudha ChakrabortyÎncă nu există evaluări
- 12 - Abylaikhan Et AlDocument11 pagini12 - Abylaikhan Et Alisti winarniÎncă nu există evaluări
- Sacks SSCTDocument25 paginiSacks SSCTEmer Son80% (5)
- SMART Goal WorksheetDocument4 paginiSMART Goal WorksheetJaskiran KaurÎncă nu există evaluări
- I. Suicide: Maria Elizabeth MendozaDocument2 paginiI. Suicide: Maria Elizabeth MendozaToshaMendozaÎncă nu există evaluări
- Interpersonal Psychotherapy For Depression Ipt Competency FrameworkDocument38 paginiInterpersonal Psychotherapy For Depression Ipt Competency FrameworkIoana Boca100% (1)
- 2014 Edwards Schemas in Clinical PracticeDocument5 pagini2014 Edwards Schemas in Clinical PracticeDavid EdwardsÎncă nu există evaluări
- Drama techniques boost learningDocument19 paginiDrama techniques boost learningDanielaRăducănescu100% (3)
- Social Anxiety TheoryDocument78 paginiSocial Anxiety TheoryAdeel Akhtar100% (2)
- Five DysfunctionsDocument1 paginăFive DysfunctionsanupsarkÎncă nu există evaluări
- Theory X & Theory Y CaseDocument7 paginiTheory X & Theory Y CasealperguzelÎncă nu există evaluări
- The Coping Circumplex Model: An Integrative Model of The Structure of Coping With StressDocument23 paginiThe Coping Circumplex Model: An Integrative Model of The Structure of Coping With StressChandanaÎncă nu există evaluări
- John Bernard Taylor Safety CultureDocument231 paginiJohn Bernard Taylor Safety Culturekusumawardati100% (2)
- Wit, H. F. de - The Case For Contemplative PsychologyDocument5 paginiWit, H. F. de - The Case For Contemplative PsychologyExopolitics ChileÎncă nu există evaluări
- Group 3 Chapter 1Document7 paginiGroup 3 Chapter 1Mavel DesamparadoÎncă nu există evaluări
- Recognizing and Responding To Anxiety in The ClassroomDocument39 paginiRecognizing and Responding To Anxiety in The ClassroomItaÎncă nu există evaluări
- Jean Piaget 4 StagesDocument2 paginiJean Piaget 4 StagesYogi YogiÎncă nu există evaluări
- Build Your Social Confidence", A Social Anxiety Group For CollegeDocument17 paginiBuild Your Social Confidence", A Social Anxiety Group For CollegejuaromerÎncă nu există evaluări
- Creative Movement TherapyDocument4 paginiCreative Movement TherapyNupur NatarajaÎncă nu există evaluări
- The Neuroscience of Dissociative Identity DisorderDocument3 paginiThe Neuroscience of Dissociative Identity DisorderdojabrÎncă nu există evaluări
- Definition Scope of Educational Psychologyu-Converted-MergedDocument385 paginiDefinition Scope of Educational Psychologyu-Converted-MergedBisma ShafiqÎncă nu există evaluări
- The Secret Lives of Wives (Newsweek 7-12-2004 Issue)Document13 paginiThe Secret Lives of Wives (Newsweek 7-12-2004 Issue)KAW88% (8)
- HRM 7Document27 paginiHRM 7Rohit VermaÎncă nu există evaluări
- HR PPT SubhajitDocument8 paginiHR PPT SubhajitSubhajit BiswasÎncă nu există evaluări
- Perkins' Exhib Summ Assess Rubric 2011Document2 paginiPerkins' Exhib Summ Assess Rubric 2011ZetsukeÎncă nu există evaluări
- Adult ADHD Self-Report Scale (ASRS-v1.1) Symptom Checklist InstructionsDocument3 paginiAdult ADHD Self-Report Scale (ASRS-v1.1) Symptom Checklist InstructionsPrivate InformationÎncă nu există evaluări
- What It Takes To Be An EntrepreneurDocument3 paginiWhat It Takes To Be An EntrepreneurJose FrancisÎncă nu există evaluări
- Howard Becker - Becoming A Marihuana UserDocument5 paginiHoward Becker - Becoming A Marihuana Userbkaplan452Încă nu există evaluări
- Job Satisfaction - NurseDocument13 paginiJob Satisfaction - NurseSivaneswary100% (1)
- Compassion-Bridging Practice and Science PDFDocument531 paginiCompassion-Bridging Practice and Science PDFjevoisarbreÎncă nu există evaluări