S-ar putea să vă placă și
- CPN Guide 2Document4 paginiCPN Guide 2Aut Beat95% (37)
- Interested Party: The Standard On West Dallas: ConfirmationDocument1 paginăInterested Party: The Standard On West Dallas: ConfirmationDaniel Lee Eisenberg JacobsÎncă nu există evaluări
- Adjusting Entries Quiz - Accounting CoachDocument4 paginiAdjusting Entries Quiz - Accounting CoachSudip BhattacharyaÎncă nu există evaluări
- CFC - Inclusive Econ ReportDocument71 paginiCFC - Inclusive Econ ReportKelly KenoyerÎncă nu există evaluări
- Moody's Upgrades To Aaa Carroll County's (MD) GO Bonds Outlook StableDocument4 paginiMoody's Upgrades To Aaa Carroll County's (MD) GO Bonds Outlook StableChris SwamÎncă nu există evaluări
- SAP FICA Configuration Step by StepDocument32 paginiSAP FICA Configuration Step by StepSourav Kumar Jena50% (4)
- Collection Notes by ClangDocument19 paginiCollection Notes by ClangQuevyn Kohl SurbanÎncă nu există evaluări
- Navigation Update User Guide: Business Team 2 Hyundai Mnsoft DEC, 2020Document89 paginiNavigation Update User Guide: Business Team 2 Hyundai Mnsoft DEC, 2020bakchoÎncă nu există evaluări
- Avanse App Form PDFDocument4 paginiAvanse App Form PDFSuresh DhanasekarÎncă nu există evaluări
- Discover Bank ReviewDocument7 paginiDiscover Bank ReviewyadavrajeÎncă nu există evaluări
- Volvo Eicher JointventureDocument11 paginiVolvo Eicher JointventureBhavini64Încă nu există evaluări
- Your Reliance Communications Bill: Summary of Current Charges Amount (RS.) 1. Monthly Rental 500.00 2. Taxes 51.50Document2 paginiYour Reliance Communications Bill: Summary of Current Charges Amount (RS.) 1. Monthly Rental 500.00 2. Taxes 51.50Vel MuruganÎncă nu există evaluări
- January 27, 2023 February 14, 2023: Credit Card StatementDocument4 paginiJanuary 27, 2023 February 14, 2023: Credit Card StatementManas MishraÎncă nu există evaluări
- Acknowledgement Receipt 20190526 151008Document2 paginiAcknowledgement Receipt 20190526 151008Arman PenalosaÎncă nu există evaluări
- Verizon Financial Analysis - FinalDocument9 paginiVerizon Financial Analysis - Finalapi-257340526Încă nu există evaluări
- Chapter 10: Personal Loans and Purchasing DecisionsDocument44 paginiChapter 10: Personal Loans and Purchasing DecisionstrishÎncă nu există evaluări
- Retail Installment Contract TemplateDocument4 paginiRetail Installment Contract TemplatenathaliaanitaÎncă nu există evaluări
- Manage Beneficiaries TIAA BankDocument2 paginiManage Beneficiaries TIAA BankAbdy Fernando SanchezÎncă nu există evaluări
- WelcomeLetter 3396301000001791Document2 paginiWelcomeLetter 3396301000001791Usman Saeed KhanÎncă nu există evaluări
- CRISIL Registration StepsDocument1 paginăCRISIL Registration StepsMarty RodriguezÎncă nu există evaluări
- Equity MarketDocument105 paginiEquity MarketSidhant ChoudhuryÎncă nu există evaluări
- Valand Rutvik Jitendrakumar 2022-08-04-07-43 Incomplete Application PDFDocument10 paginiValand Rutvik Jitendrakumar 2022-08-04-07-43 Incomplete Application PDFTestÎncă nu există evaluări
- LIT 7143614 Nov-23 UnlockedDocument3 paginiLIT 7143614 Nov-23 Unlockedhdfccreditcard328Încă nu există evaluări
- Loan Term Sheet - 20 - 12 - 42Document21 paginiLoan Term Sheet - 20 - 12 - 42Md riyaj ali KhanÎncă nu există evaluări
- CAMSKRA Individual FormDocument2 paginiCAMSKRA Individual FormavnayakÎncă nu există evaluări
- Payment Schedule - 20190430 - 073337 PDFDocument2 paginiPayment Schedule - 20190430 - 073337 PDFKylyn JynÎncă nu există evaluări
- AT&T Customer Service SummaryDocument1 paginăAT&T Customer Service SummaryHector VillavicencioÎncă nu există evaluări
- Verizon Voice Plans 2010Document1 paginăVerizon Voice Plans 2010kpal525Încă nu există evaluări
- Medical Insurance 2020Document4 paginiMedical Insurance 2020Victor WongÎncă nu există evaluări
- Falcon Price Book Revised 8/13Document278 paginiFalcon Price Book Revised 8/13Security Lock DistributorsÎncă nu există evaluări
- Setting Up SMS Sending and Receiving Using A USB GSM Dongle by ZTE - Selective IntellectDocument15 paginiSetting Up SMS Sending and Receiving Using A USB GSM Dongle by ZTE - Selective IntellectlordkurÎncă nu există evaluări
- Hong Kong: Travel Briefing For Transfer On Work PermitDocument24 paginiHong Kong: Travel Briefing For Transfer On Work PermitrajeshmsitÎncă nu există evaluări
- Ethiopia, 6.625% 11dec2024, USDDocument1 paginăEthiopia, 6.625% 11dec2024, USDLloyd Ki'sÎncă nu există evaluări
- Project 2022Document84 paginiProject 2022Shriya Vikram ShahÎncă nu există evaluări
- Territoial Army Officers Recruitment 2023 NotificationDocument3 paginiTerritoial Army Officers Recruitment 2023 Notificationsrimanta kumar baradÎncă nu există evaluări
- Xyz 64070982438Document1 paginăXyz 64070982438Niro ViroÎncă nu există evaluări
- EPGP 2024 25v9Document4 paginiEPGP 2024 25v9ARUN MUNOLIÎncă nu există evaluări
- Alternative Education Center at LamarDocument4 paginiAlternative Education Center at LamarJeremy TurnageÎncă nu există evaluări
- SampleNAB Statement X7819 26-Oct-2021Document10 paginiSampleNAB Statement X7819 26-Oct-2021Tobias PriceÎncă nu există evaluări
- ht2000w PDFDocument12 paginiht2000w PDFThiha KyawÎncă nu există evaluări
- (Ddau Am (E (Ê$.) : (NN BM H$M'M WJVMZ Es Oñq - Q G DV© - MZ Ewëh$ HW$B Xo' Am (E WJVMZ Xo' (V (WDocument5 pagini(Ddau Am (E (Ê$.) : (NN BM H$M'M WJVMZ Es Oñq - Q G DV© - MZ Ewëh$ HW$B Xo' Am (E WJVMZ Xo' (V (WDeepak DahiyaÎncă nu există evaluări
- AG Letitia James Against Uri Koenig & Efraim Steif, Van Duyn Owners (Doc 1)Document20 paginiAG Letitia James Against Uri Koenig & Efraim Steif, Van Duyn Owners (Doc 1)Desiree YaganÎncă nu există evaluări
- Invoice 317854Document3 paginiInvoice 317854Catalina MititelÎncă nu există evaluări
- M240i AutoCheckDocument5 paginiM240i AutoCheckSUHIMAN SALMANÎncă nu există evaluări
- Fiber Monthly Statement: This Month's SummaryDocument4 paginiFiber Monthly Statement: This Month's Summaryavinash kumarÎncă nu există evaluări
- Summer School Session-Registration RegsDocument4 paginiSummer School Session-Registration RegsShanica Paul-RichardsÎncă nu există evaluări
- VQ.23 04343 3Document3 paginiVQ.23 04343 3tdm_101Încă nu există evaluări
- SBM Onecard Lite TCsDocument28 paginiSBM Onecard Lite TCsRAJ KUMHAREÎncă nu există evaluări
- Egov Urban Portal-Water Tax PDFDocument2 paginiEgov Urban Portal-Water Tax PDFPadmavathi Putra LokeshÎncă nu există evaluări
- Monthly Services: Included at No Extra CostDocument1 paginăMonthly Services: Included at No Extra CostRajnish VermaÎncă nu există evaluări
- What Is Insurance Full Details PRE VS POST COVID by VishalDocument13 paginiWhat Is Insurance Full Details PRE VS POST COVID by VishalVishalÎncă nu există evaluări
- Education 11 00462Document13 paginiEducation 11 00462Ashlyn AlmacenÎncă nu există evaluări
- Fhava Amendatory Clause 1221 ts50096Document1 paginăFhava Amendatory Clause 1221 ts50096EdgarÎncă nu există evaluări
- Emami Fashion 2015 ETBDocument85 paginiEmami Fashion 2015 ETBAnanda Satyam MaheswarnathÎncă nu există evaluări
- Receipt PDFDocument2 paginiReceipt PDFMicah StapleÎncă nu există evaluări
- Austin Yaw Ansah Akuffo-Organizational Behavior Assignement - Task 3Document12 paginiAustin Yaw Ansah Akuffo-Organizational Behavior Assignement - Task 3Nana Akufo AnsahÎncă nu există evaluări
- Sep2023Document8 paginiSep2023Sushmitha ThulasimaniÎncă nu există evaluări
- Somerset Homes For Sale 200-250kDocument24 paginiSomerset Homes For Sale 200-250kSuzanne SandsÎncă nu există evaluări
- DownloadDocument5 paginiDownloadRISHABHÎncă nu există evaluări
- MMT Platinum TNCDocument9 paginiMMT Platinum TNCezaza3108Încă nu există evaluări
- FAM Funds 2020 Annual LetterDocument9 paginiFAM Funds 2020 Annual LetterYog MehtaÎncă nu există evaluări
- Ymca Camp Permission & Health Form: Additional Authorized Persons For Pick UpDocument4 paginiYmca Camp Permission & Health Form: Additional Authorized Persons For Pick Upahcobras1314Încă nu există evaluări
- 2012 Camp TEKO Registration FormDocument2 pagini2012 Camp TEKO Registration FormAndrea GordonÎncă nu există evaluări
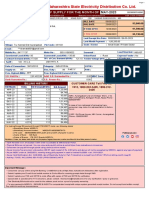
- Bill of Supply For The Month of Mar 2019: Maharashtra State Electricity Distribution Co - LTDDocument3 paginiBill of Supply For The Month of Mar 2019: Maharashtra State Electricity Distribution Co - LTDJyotsna TandelÎncă nu există evaluări
- Gifts - Ie Christmas Hamper Brochure 2007Document24 paginiGifts - Ie Christmas Hamper Brochure 2007gifts.ie100% (1)
- PDF Presenter NotesDocument14 paginiPDF Presenter NotesYu EnÎncă nu există evaluări
- Acosj-P: Java Card - PBOC 3.0Document22 paginiAcosj-P: Java Card - PBOC 3.0Alfi AlirezaÎncă nu există evaluări
- RD050 Fixed AssetDocument33 paginiRD050 Fixed Assetnahmedicsm7048Încă nu există evaluări
- Business 2257 Tutorial #2Document17 paginiBusiness 2257 Tutorial #2westernbebeÎncă nu există evaluări
- Group 2A: Catanduanes State University Calatagan Virac, CatanduanesDocument9 paginiGroup 2A: Catanduanes State University Calatagan Virac, CatanduanesLaila Mae PiloneoÎncă nu există evaluări
- Bill 670 502039075170 202305Document5 paginiBill 670 502039075170 202305pravin ghatgeÎncă nu există evaluări
- Doremi Partnership: Do, Capital (20%) Re, Capital (30%) Mi, Capital (50%)Document4 paginiDoremi Partnership: Do, Capital (20%) Re, Capital (30%) Mi, Capital (50%)Guiana WacasÎncă nu există evaluări
- Make Model Body Type: Bill of Sale of Automobile New York County ofDocument3 paginiMake Model Body Type: Bill of Sale of Automobile New York County ofDee ChhabraÎncă nu există evaluări
- Pentagon - IDBI 000569 - NovDocument58 paginiPentagon - IDBI 000569 - NovnaniÎncă nu există evaluări
- Horizon Trial: Day 3 Aakash Patny Witness StatementDocument4 paginiHorizon Trial: Day 3 Aakash Patny Witness StatementNick WallisÎncă nu există evaluări
- English Institute in Hyderabad IndiaDocument17 paginiEnglish Institute in Hyderabad Indialavkush tripathiÎncă nu există evaluări
- Sno Description Quantity Rate Amount: Proforma InvoiceDocument1 paginăSno Description Quantity Rate Amount: Proforma InvoiceMEDICAL SUPERINTENDENTÎncă nu există evaluări
- Detailed Instructions For Applying To SWPS University 2020-2021 EngDocument4 paginiDetailed Instructions For Applying To SWPS University 2020-2021 EngBest SelectÎncă nu există evaluări
- AblDocument19 paginiAblSaad RajaÎncă nu există evaluări
- Iit Jee Study MaterialDocument3 paginiIit Jee Study MaterialIit - PulseÎncă nu există evaluări
- BSP Memorandum 2018-21Document8 paginiBSP Memorandum 2018-21Maya Julieta Catacutan-EstabilloÎncă nu există evaluări
- TENMET Financial PoliciesDocument48 paginiTENMET Financial PoliciesFrank AllanÎncă nu există evaluări
- DealposDocument19 paginiDealposBli RiyanÎncă nu există evaluări
- Urgent Application-For-CgsDocument5 paginiUrgent Application-For-CgsTharaka Nuwan100% (1)
- ResumeDocument7 paginiResumetomjos66100% (2)
- Pmi Order 28000162695Document1 paginăPmi Order 28000162695salahadinÎncă nu există evaluări
- Internship Report On Global Ime Bank Limited: Submitted By: Niraj Lamsal Exam Roll No: MU Reg. NoDocument37 paginiInternship Report On Global Ime Bank Limited: Submitted By: Niraj Lamsal Exam Roll No: MU Reg. NoNiraj LamsalÎncă nu există evaluări
- Bhagya Viva ProjectDocument13 paginiBhagya Viva ProjectBhagya sÎncă nu există evaluări
- SIDBI Recruitment of Officers in Grade A'-General Stream 2016Document21 paginiSIDBI Recruitment of Officers in Grade A'-General Stream 2016Manjunath HSÎncă nu există evaluări