S-ar putea să vă placă și
- Benign Prostatic Hypertrophy: A Beginner's 3-Step Plan for Managing BPH With Diet and Nutrition, with Sample Recipes and a Meal PlanDe la EverandBenign Prostatic Hypertrophy: A Beginner's 3-Step Plan for Managing BPH With Diet and Nutrition, with Sample Recipes and a Meal PlanÎncă nu există evaluări
- BPH JurnalDocument35 paginiBPH Jurnalrevina_revi0% (2)
- Dutasteride 0.5mg (Avodart)Document14 paginiDutasteride 0.5mg (Avodart)ddandan_2Încă nu există evaluări
- Current Status of 5 of Lower Urinary Tract Symptoms and BPH: - Reductase Inhibitors in The ManagementDocument8 paginiCurrent Status of 5 of Lower Urinary Tract Symptoms and BPH: - Reductase Inhibitors in The ManagementApriani BahoriÎncă nu există evaluări
- Duodart: Dutasteride-Tamsulosin HydrochlorideDocument23 paginiDuodart: Dutasteride-Tamsulosin HydrochlorideYessy AndikaÎncă nu există evaluări
- Benign Prostatic HypertrophyDocument3 paginiBenign Prostatic HypertrophyDjdjjd SiisusÎncă nu există evaluări
- Kim 2017Document5 paginiKim 2017kanaÎncă nu există evaluări
- BPH Smith English-6-15Document10 paginiBPH Smith English-6-15novi camiumÎncă nu există evaluări
- Benign Prostatic Hypertrophy: An Update On Drug TherapyDocument2 paginiBenign Prostatic Hypertrophy: An Update On Drug TherapyAjieRnie IDÎncă nu există evaluări
- Dutasteride 0.5mg + Tamsulosin HCL 0.4mg (Duodart)Document19 paginiDutasteride 0.5mg + Tamsulosin HCL 0.4mg (Duodart)ddandan_2Încă nu există evaluări
- Benign Prostatic: Hypertrophy Hyperplasia EnlargementDocument40 paginiBenign Prostatic: Hypertrophy Hyperplasia EnlargementAyu PurbaÎncă nu există evaluări
- Medical Therapy For Benign Prostatic Hyperplasia: A ReviewDocument11 paginiMedical Therapy For Benign Prostatic Hyperplasia: A ReviewEfson Sustera IrawanÎncă nu există evaluări
- Tamsulosin - Drug Information - UpToDateDocument23 paginiTamsulosin - Drug Information - UpToDateGénesis GabrielaÎncă nu există evaluări
- Fixed-Dose Combination Therapy With Dutasteride AnDocument10 paginiFixed-Dose Combination Therapy With Dutasteride AnsyukronchalimÎncă nu există evaluări
- BPH NotesDocument6 paginiBPH NotesLorina ApelacioÎncă nu există evaluări
- Combination Medical Therapy For Lower Urinary Tract Symptoms and Benign Prostatic HyperplasiaDocument9 paginiCombination Medical Therapy For Lower Urinary Tract Symptoms and Benign Prostatic HyperplasiaganangahimsaÎncă nu există evaluări
- BPE Happens When The Number of Cells in The Prostate IncreasesDocument4 paginiBPE Happens When The Number of Cells in The Prostate Increasesrasnamj009Încă nu există evaluări
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument12 paginiSummary of Product Characteristics: 4.1 Therapeutic IndicationsAEE MHCH Sub Div 1stÎncă nu există evaluări
- TCRM 5 535Document11 paginiTCRM 5 535ganangahimsaÎncă nu există evaluări
- CombatDocument9 paginiCombatMIHAELAÎncă nu există evaluări
- MADRAC Bulletin August 2011Document12 paginiMADRAC Bulletin August 2011CrocStickerÎncă nu există evaluări
- Roehrborn Et al-2015-BJU InternationalDocument10 paginiRoehrborn Et al-2015-BJU InternationalyuenkeithÎncă nu există evaluări
- Drug StudyDocument5 paginiDrug StudySmol PadernalÎncă nu există evaluări
- Patient Education HPBDocument9 paginiPatient Education HPBSALOME PANTOJAÎncă nu există evaluări
- BPH - Muh ShilahulDocument3 paginiBPH - Muh ShilahulshilchanÎncă nu există evaluări
- Reduce TrialDocument7 paginiReduce TrialTong YangaÎncă nu există evaluări
- Apo Prazosin PiDocument9 paginiApo Prazosin PiNadya UtariÎncă nu există evaluări
- Finasteride in The Treatment of Patients BPHDocument11 paginiFinasteride in The Treatment of Patients BPHmonia agni wiyatamiÎncă nu există evaluări
- Benign Prostatic HyperplasiaDocument16 paginiBenign Prostatic HyperplasiaJood AL AbriÎncă nu există evaluări
- Benign Prostatic HyperplasiaDocument29 paginiBenign Prostatic HyperplasiaYoseph Alam NaibahoÎncă nu există evaluări
- PEER Stage2 10.1038 Pcan.2011.13 PDFDocument22 paginiPEER Stage2 10.1038 Pcan.2011.13 PDFMIHAELAÎncă nu există evaluări
- New Zealand Data Sheet: PresentationDocument6 paginiNew Zealand Data Sheet: PresentationSudhir SinghÎncă nu există evaluări
- Palacios 2006Document11 paginiPalacios 2006perezhuertalexieÎncă nu există evaluări
- Tamsulosin SOLDocument18 paginiTamsulosin SOLdr.yogaÎncă nu există evaluări
- WJBPHS 2023 0299Document6 paginiWJBPHS 2023 0299Luana AraújoÎncă nu există evaluări
- Silodosin Versus Tamsulosin in Symptomatic Benign Prostatic Hyperplasia-Our ExperienceDocument3 paginiSilodosin Versus Tamsulosin in Symptomatic Benign Prostatic Hyperplasia-Our ExperienceIOSR Journal of PharmacyÎncă nu există evaluări
- Testosterone Replacement TherapyDocument4 paginiTestosterone Replacement Therapyall-testosteroneÎncă nu există evaluări
- 1 s2.0 S2049080122008974 MainDocument4 pagini1 s2.0 S2049080122008974 MainGregory AssonitisÎncă nu există evaluări
- Finasteride 5 MG Tablets - Summary of Product Characteristics (SPC) - (eMC)Document6 paginiFinasteride 5 MG Tablets - Summary of Product Characteristics (SPC) - (eMC)neleatucicovshiiÎncă nu există evaluări
- BPH Medication BUUDocument33 paginiBPH Medication BUUWisnu TirtayasaÎncă nu există evaluări
- Saw Palmetto For Prostate DisordersDocument3 paginiSaw Palmetto For Prostate Disordersahmadslayman1Încă nu există evaluări
- A Critical Review of CernitinDocument10 paginiA Critical Review of Cernitinnadamau22633Încă nu există evaluări
- Farmakoterapi Inkontinensia Urin, Enuresis, BPHDocument43 paginiFarmakoterapi Inkontinensia Urin, Enuresis, BPHAnastasya LunasikifaÎncă nu există evaluări
- Drug Interaction Report Agust 17 KosimDocument5 paginiDrug Interaction Report Agust 17 KosimarifÎncă nu există evaluări
- Pharma ProjectDocument9 paginiPharma Projectfarah.abd97Încă nu există evaluări
- Indian Herbs That Act As 5-Alpha Reductase InhibitorsDocument9 paginiIndian Herbs That Act As 5-Alpha Reductase InhibitorsMan ManÎncă nu există evaluări
- BPH JournalDocument8 paginiBPH JournalJuliaÎncă nu există evaluări
- Femara: (Letrozole Tablets) 2.5 MG Tablets RX Only Prescribing InformationDocument28 paginiFemara: (Letrozole Tablets) 2.5 MG Tablets RX Only Prescribing InformationKirubakaranÎncă nu există evaluări
- Canuuc - Prostate Disease 1 Benign May 2017Document29 paginiCanuuc - Prostate Disease 1 Benign May 2017dktkaÎncă nu există evaluări
- Benign Prostatic HyperplasiaDocument18 paginiBenign Prostatic HyperplasiaGunawan SadewoÎncă nu există evaluări
- BPH InternetDocument72 paginiBPH InternetDesty ArianiÎncă nu există evaluări
- Benign Prostat HiperplasiaDocument17 paginiBenign Prostat HiperplasiahawhawnurÎncă nu există evaluări
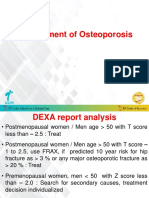
- Management of OsteoporosisDocument35 paginiManagement of OsteoporosisAKSHAT GARGÎncă nu există evaluări
- 2014 Prostate Cancer BRIEFDocument1 pagină2014 Prostate Cancer BRIEFsalva1310Încă nu există evaluări
- Hamed Alabad BPHDocument47 paginiHamed Alabad BPHHamed AlabadÎncă nu există evaluări
- Benign Prostatic Hyperplasia (BPH)Document88 paginiBenign Prostatic Hyperplasia (BPH)Hussein AlhaddadÎncă nu există evaluări
- 15 5a-Reductase Inhibitors in Benign Prostatic Hyperplasia and Prostate Cancer Risk ReductionDocument14 pagini15 5a-Reductase Inhibitors in Benign Prostatic Hyperplasia and Prostate Cancer Risk ReductionDr-Mandeep SinghÎncă nu există evaluări
- Benign Prostatic Hypertrophy Comprehensive Management Guide 2Document9 paginiBenign Prostatic Hypertrophy Comprehensive Management Guide 2Thanakorn WongsombutÎncă nu există evaluări
- Analgesic: Mefenamic AcidDocument5 paginiAnalgesic: Mefenamic Acidmegazhang94Încă nu există evaluări
- Primary and Secondary Prevention of Benign Prostatic HyperplasiaDocument2 paginiPrimary and Secondary Prevention of Benign Prostatic HyperplasiaNina MelinaÎncă nu există evaluări
- Strategic Plan 2023Document12 paginiStrategic Plan 2023BernewsAdminÎncă nu există evaluări
- Logical Reasoning Sectional TestDocument15 paginiLogical Reasoning Sectional TestAditya HiremathÎncă nu există evaluări
- (PDF) Pass Through Panic: Freeing Yourself From Anxiety and FearDocument1 pagină(PDF) Pass Through Panic: Freeing Yourself From Anxiety and FearmilonÎncă nu există evaluări
- J Applied Clin Med Phys - 2022 - Fisher - AAPM Medical Physics Practice Guideline 12 A Fluoroscopy Dose Management-1Document19 paginiJ Applied Clin Med Phys - 2022 - Fisher - AAPM Medical Physics Practice Guideline 12 A Fluoroscopy Dose Management-1Roshi_11Încă nu există evaluări
- Technical Publications: Revision 5Document104 paginiTechnical Publications: Revision 5Maciel RamosÎncă nu există evaluări
- MT-Mental Health-JMTDocument29 paginiMT-Mental Health-JMTLuis AlbertoÎncă nu există evaluări
- Alimentos PH Urinario GatosDocument4 paginiAlimentos PH Urinario GatosLarissa VianaÎncă nu există evaluări
- SF2 - 2020 - Grade 6 - MALINISDocument2 paginiSF2 - 2020 - Grade 6 - MALINISJerson S. SantiagoÎncă nu există evaluări
- Mapeh 8-2ND Semi QuarterDocument5 paginiMapeh 8-2ND Semi QuarterQueenie GamboaÎncă nu există evaluări
- Local Food Trade Shows ProgramDocument39 paginiLocal Food Trade Shows ProgramAmy KleinÎncă nu există evaluări
- How To Write Clinical Learning ObjectivesDocument1 paginăHow To Write Clinical Learning ObjectivesNick MacaballugÎncă nu există evaluări
- Lab1ESR 08Document11 paginiLab1ESR 08Muhamad AfidinÎncă nu există evaluări
- AllianzDocument27 paginiAllianzHariz SyahmiÎncă nu există evaluări
- Black SigatokaDocument2 paginiBlack SigatokaLALUKISÎncă nu există evaluări
- FSCC 22000 Version 5 and Other RequirementsDocument29 paginiFSCC 22000 Version 5 and Other Requirementskrishan100% (1)
- Cartoon DivingDocument7 paginiCartoon Divingapi-321333695Încă nu există evaluări
- CP 576Document8 paginiCP 576MMM-2012Încă nu există evaluări
- Parkinsonism A General Motor Disability PDFDocument9 paginiParkinsonism A General Motor Disability PDFRishabh SinghÎncă nu există evaluări
- Rallygram 2022 FinalDocument4 paginiRallygram 2022 Finalapi-654829982Încă nu există evaluări
- Fispq Pta - Pqs EnglishDocument11 paginiFispq Pta - Pqs EnglishRisad She NappholeontÎncă nu există evaluări
- CF 756Document100 paginiCF 756Manoj KumarÎncă nu există evaluări
- Dela Rosa, S1 - Ep11Document1 paginăDela Rosa, S1 - Ep11Marjorie Dela RosaÎncă nu există evaluări
- Contoh Daftar Belanja Obat Praktek PribadiDocument10 paginiContoh Daftar Belanja Obat Praktek PribadimeryÎncă nu există evaluări
- Hbsag Form New 2021Document1 paginăHbsag Form New 2021GCMDHÎncă nu există evaluări
- 1a.3 - Bridge Watchkeeping LevelsDocument8 pagini1a.3 - Bridge Watchkeeping LevelsRaghav SoodÎncă nu există evaluări
- Manual For Doctors To Evaluate Permanent Physical ImpairmentDocument33 paginiManual For Doctors To Evaluate Permanent Physical Impairmentyuvrajavi100% (1)
- National Political Parties in India: Hidayatullah National Law University Raipur, ChhattisgarhDocument34 paginiNational Political Parties in India: Hidayatullah National Law University Raipur, ChhattisgarhshiviÎncă nu există evaluări
- Construction and Validation of PS-FFQ (Parenting Style Four Factor Questionnaire)Document12 paginiConstruction and Validation of PS-FFQ (Parenting Style Four Factor Questionnaire)Bernard CarpioÎncă nu există evaluări
- Pathophysiology For Health Sciences BHS415: Rozzana Mohd Said, PHDDocument20 paginiPathophysiology For Health Sciences BHS415: Rozzana Mohd Said, PHDatiqullah tarmiziÎncă nu există evaluări
- Specific Lifting Pland - OHS-PR-009 - FM-01-051. Rv2Document2 paginiSpecific Lifting Pland - OHS-PR-009 - FM-01-051. Rv2cmrig74Încă nu există evaluări
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (29)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Evaluare: 3 din 5 stele3/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (5)
- Troubled: A Memoir of Foster Care, Family, and Social ClassDe la EverandTroubled: A Memoir of Foster Care, Family, and Social ClassEvaluare: 4.5 din 5 stele4.5/5 (27)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 4 din 5 stele4/5 (4)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (59)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (45)