S-ar putea să vă placă și
- Harv Life SC Data SCDocument5 paginiHarv Life SC Data SCLavina D'costaÎncă nu există evaluări
- Chapter 7 EvolutionDocument17 paginiChapter 7 EvolutionLavina D'costaÎncă nu există evaluări
- NCERT Solutions Class 12th Biology: Chapter 9 - Strategies For Enhancement in Food ProductionDocument7 paginiNCERT Solutions Class 12th Biology: Chapter 9 - Strategies For Enhancement in Food ProductionLavina D'costaÎncă nu există evaluări
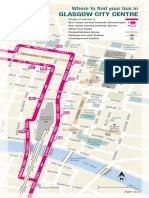
- Glasgow City Centre: Where To Find Your Bus inDocument3 paginiGlasgow City Centre: Where To Find Your Bus inLavina D'costaÎncă nu există evaluări
- Gut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceDocument21 paginiGut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceLavina D'costaÎncă nu există evaluări
- Chapter 3Document8 paginiChapter 3Lavina D'costaÎncă nu există evaluări
- Mitochondrial DNA VariatnDocument6 paginiMitochondrial DNA VariatnLavina D'costaÎncă nu există evaluări
- B Hler Et Al 1998 Yeast 2Document9 paginiB Hler Et Al 1998 Yeast 2Lavina D'costaÎncă nu există evaluări
- Cell Cycle M SmegDocument15 paginiCell Cycle M SmegLavina D'costaÎncă nu există evaluări
- Transcriptional Profiling of BladderDocument13 paginiTranscriptional Profiling of BladderLavina D'costaÎncă nu există evaluări
- Immuno PathologyDocument13 paginiImmuno PathologyLavina D'costaÎncă nu există evaluări
- Regulation of Expression, Function, and inDocument9 paginiRegulation of Expression, Function, and inLavina D'costaÎncă nu există evaluări
- Microbiology Lab BookDocument83 paginiMicrobiology Lab BookLavina D'costa100% (6)
- Lactobacillus Probiotic Protects Intestinal EpitheliumDocument12 paginiLactobacillus Probiotic Protects Intestinal EpitheliumLavina D'costaÎncă nu există evaluări
- Trafficking of Endosomal Toll-LikeDocument10 paginiTrafficking of Endosomal Toll-LikeLavina D'costaÎncă nu există evaluări
- Benefits of Caffeine Citrate - Neurodevelopmental Outcomes of ELBDocument15 paginiBenefits of Caffeine Citrate - Neurodevelopmental Outcomes of ELBLavina D'costaÎncă nu există evaluări
- The Toll-Like Receptor Pathway Establishes Commensal Gut ColonizationDocument14 paginiThe Toll-Like Receptor Pathway Establishes Commensal Gut ColonizationLavina D'costaÎncă nu există evaluări
- Expression of Microbiota, Toll Like Receptors,& Regulators in SmallDocument6 paginiExpression of Microbiota, Toll Like Receptors,& Regulators in SmallLavina D'costaÎncă nu există evaluări
- Phylo PDFDocument20 paginiPhylo PDFLavina D'costaÎncă nu există evaluări
- Gut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceDocument21 paginiGut Microbiota Is A Key Modulator of Insulin Resistance in TLR2 Def MiceLavina D'costaÎncă nu există evaluări
- Colorazione Ziehl NeelsenDocument4 paginiColorazione Ziehl NeelsenLavina D'costaÎncă nu există evaluări
- Does TLR2 Regulate Intestinal InflammationDocument3 paginiDoes TLR2 Regulate Intestinal InflammationLavina D'costaÎncă nu există evaluări
- Chapter 4: Diagnosis of TB DiseaseDocument34 paginiChapter 4: Diagnosis of TB DiseaseROHITÎncă nu există evaluări
- Phylo PDFDocument20 paginiPhylo PDFLavina D'costaÎncă nu există evaluări
- 21 24 PDFDocument4 pagini21 24 PDFLavina D'costaÎncă nu există evaluări
- Medicinal Uses For CorianderDocument2 paginiMedicinal Uses For CorianderLavina D'costaÎncă nu există evaluări
- Phylo PDFDocument20 paginiPhylo PDFLavina D'costaÎncă nu există evaluări
- 2009 MMTV Like and Diagnostic Value N Human BR Ca PDFDocument31 pagini2009 MMTV Like and Diagnostic Value N Human BR Ca PDFLavina D'costaÎncă nu există evaluări
- GRE Screen Reader InstructionsDocument4 paginiGRE Screen Reader InstructionsWaheed UllahÎncă nu există evaluări
- Agglutinin From Arachis Hypogaea: Site-Specific Monoclonal Antibodies Against PeanutDocument10 paginiAgglutinin From Arachis Hypogaea: Site-Specific Monoclonal Antibodies Against PeanutLavina D'costaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Women &literatureDocument54 paginiWomen &literatureAicha ZianeÎncă nu există evaluări
- Organizational Development ProcessDocument1 paginăOrganizational Development ProcessMohit SharmaÎncă nu există evaluări
- Benchmark Evidence BasedDocument11 paginiBenchmark Evidence BasedPeterÎncă nu există evaluări
- Tait V MSAD 61 ComplaintDocument36 paginiTait V MSAD 61 ComplaintNEWS CENTER MaineÎncă nu există evaluări
- Cheap Shots Ambushes and Other Lessons Marc Animal MacYoung DjvuDocument179 paginiCheap Shots Ambushes and Other Lessons Marc Animal MacYoung DjvuСергей Фомин100% (1)
- Genealogy On June 09-2003Document25 paginiGenealogy On June 09-2003syedyusufsam92100% (3)
- Flow Through AnnulusDocument7 paginiFlow Through Annulusamir_hayfaÎncă nu există evaluări
- An Exploratory Study of Personal Calendar UseDocument23 paginiAn Exploratory Study of Personal Calendar UseManas Tungare100% (1)
- RICS Research On NECDocument9 paginiRICS Research On NECAhmad MajedÎncă nu există evaluări
- Pan or The DevilDocument8 paginiPan or The DevilMarguerite and Leni Johnson100% (1)
- Sylviane Granger, Gaëtanelle Gilquin, Fanny Meunier - The Cambridge Handbook of Learner Corpus Research-Cambridge University Press (2015)Document618 paginiSylviane Granger, Gaëtanelle Gilquin, Fanny Meunier - The Cambridge Handbook of Learner Corpus Research-Cambridge University Press (2015)Joyce CheungÎncă nu există evaluări
- Preparation Total Consecration PDFDocument872 paginiPreparation Total Consecration PDFgbarcelonÎncă nu există evaluări
- Understanding The SelfDocument10 paginiUnderstanding The Selfgame master50% (2)
- English - Vocabulary - in - Use - Pre - Intermediate - and - Intermediate - Book 2Document2 paginiEnglish - Vocabulary - in - Use - Pre - Intermediate - and - Intermediate - Book 2Наталия БруслинецÎncă nu există evaluări
- Pulp Fiction DeconstructionDocument3 paginiPulp Fiction Deconstructiondomatthews09Încă nu există evaluări
- Briar B. Crain: EducationDocument2 paginiBriar B. Crain: Educationapi-541610137Încă nu există evaluări
- Informative Speech 2010 (Speaking Outline) 2Document5 paginiInformative Speech 2010 (Speaking Outline) 2FaranzaSynsÎncă nu există evaluări
- Einstein AnalysisDocument2 paginiEinstein AnalysisJason LiebsonÎncă nu există evaluări
- Determinants of Cash HoldingsDocument26 paginiDeterminants of Cash Holdingspoushal100% (1)
- National Competency Based Teachers StandardDocument34 paginiNational Competency Based Teachers Standarddanebantilan100% (3)
- Fiber Optics: By: Engr. Syed Asad AliDocument20 paginiFiber Optics: By: Engr. Syed Asad Alisyedasad114Încă nu există evaluări
- Signals SyllabusDocument1 paginăSignals SyllabusproÎncă nu există evaluări
- Computerised Accounting SystemDocument14 paginiComputerised Accounting SystemramneekdadwalÎncă nu există evaluări
- Dissertation Le Juge Administratif Et Le Droit InternationalDocument8 paginiDissertation Le Juge Administratif Et Le Droit InternationalPayPeopleToWritePapersWestValleyCityÎncă nu există evaluări
- Reviewer Constitutional LawDocument6 paginiReviewer Constitutional LawMoireeGÎncă nu există evaluări
- Rietveld Made Easy - OverviewDocument3 paginiRietveld Made Easy - Overviewhp2020Încă nu există evaluări
- 00 HR Analytics 2018Document40 pagini00 HR Analytics 2018Aalya ModiÎncă nu există evaluări
- HRM in InfosysDocument11 paginiHRM in Infosysguptarahul27550% (4)
- Objective/Multiple Type QuestionDocument14 paginiObjective/Multiple Type QuestionMITALI TAKIAR100% (1)
- Student Assessment Tasks: Tasmanian State Service Senior Executive Performance Management Plan Template 1Document77 paginiStudent Assessment Tasks: Tasmanian State Service Senior Executive Performance Management Plan Template 1Imran WaheedÎncă nu există evaluări