S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Calendrical Savants: Exceptionality and Practice: Richard Cowan, Daniel P.J. CarneyDocument9 paginiCalendrical Savants: Exceptionality and Practice: Richard Cowan, Daniel P.J. CarneyKaren SaviottiÎncă nu există evaluări
- Idiot Savant Calendrical Calculators: Maths or Memory?Document6 paginiIdiot Savant Calendrical Calculators: Maths or Memory?Karen SaviottiÎncă nu există evaluări
- Do Calendrical Savants Use Calculation To Answer Date Questions? A Functional Magnetic Resonance Imaging StudyDocument8 paginiDo Calendrical Savants Use Calculation To Answer Date Questions? A Functional Magnetic Resonance Imaging StudyKaren SaviottiÎncă nu există evaluări
- The Structure of Savant Calendrical Knowledge: Developmental Medicine & Child Neurology Original ArticleDocument7 paginiThe Structure of Savant Calendrical Knowledge: Developmental Medicine & Child Neurology Original ArticleKaren SaviottiÎncă nu există evaluări
- The 'Intelligence' of Calendrical Calculators: American Journal of Mental Retardation: AJMR October 1994Document16 paginiThe 'Intelligence' of Calendrical Calculators: American Journal of Mental Retardation: AJMR October 1994Karen SaviottiÎncă nu există evaluări
- Bowen - Fields - Kensinger - InPress - BioRxiv - Valência de MemóriasDocument25 paginiBowen - Fields - Kensinger - InPress - BioRxiv - Valência de MemóriasKaren SaviottiÎncă nu există evaluări
- Developmental Outcomes and Quality of Life PDFDocument11 paginiDevelopmental Outcomes and Quality of Life PDFLucas P. TepedinoÎncă nu există evaluări
- Distinguishing Between Depression and Dementia in ElderlyDocument22 paginiDistinguishing Between Depression and Dementia in ElderlyKaren SaviottiÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Course Module EL. 107 Week 2Document22 paginiCourse Module EL. 107 Week 2Joevannie AceraÎncă nu există evaluări
- EF3e Preint Filetest 02b Answer Sheet PDFDocument1 paginăEF3e Preint Filetest 02b Answer Sheet PDFDiego Real Torres NinaÎncă nu există evaluări
- Math Anxiety Level QuestionnaireDocument12 paginiMath Anxiety Level QuestionnaireHzui FS?Încă nu există evaluări
- Module 1.1Document4 paginiModule 1.1Jen Kerly100% (2)
- Letter of Rec - Department Chair 1Document1 paginăLetter of Rec - Department Chair 1api-285300958Încă nu există evaluări
- Discourse Analysis ModuleDocument45 paginiDiscourse Analysis ModulejesuscolinaÎncă nu există evaluări
- Training Design For Career Guidance Advocacy ProgramDocument2 paginiTraining Design For Career Guidance Advocacy ProgramAyesha MeloÎncă nu există evaluări
- NEWEST!!! Competency - Framework - ENDocument44 paginiNEWEST!!! Competency - Framework - ENEka Ponkratova100% (1)
- Annotated Bibliography - Joel Kim 1Document5 paginiAnnotated Bibliography - Joel Kim 1api-316739257Încă nu există evaluări
- Work Immersion PortfolioDocument41 paginiWork Immersion PortfolioAnn Clarise Hebron BarbazaÎncă nu există evaluări
- Bristol Skills FrameworkDocument3 paginiBristol Skills FrameworkLetitia100% (1)
- Basics: Architectural Design Designing Architecture Language of Space and Form Diagramming The Big Idea and ArchitectureDocument7 paginiBasics: Architectural Design Designing Architecture Language of Space and Form Diagramming The Big Idea and ArchitectureNaveen KishoreÎncă nu există evaluări
- Japanese Style Organization and ControlDocument9 paginiJapanese Style Organization and ControlAnna DyÎncă nu există evaluări
- Motion EconomyDocument15 paginiMotion EconomySumit DhallÎncă nu există evaluări
- Portfolio Assessment RubricDocument1 paginăPortfolio Assessment RubricMarieCris67% (3)
- Comments: Sample Report CardDocument2 paginiComments: Sample Report CardLam Nguyen Truc Lam100% (2)
- HA Assessment Teachers Book B1 2Document368 paginiHA Assessment Teachers Book B1 2Надя ДерегановаÎncă nu există evaluări
- Objectives: Define Problem Posing Apply Problem Posing in Real-Life SituationDocument8 paginiObjectives: Define Problem Posing Apply Problem Posing in Real-Life SituationJang Ye HunÎncă nu există evaluări
- 04) Reading Vocabulary QuestionDocument3 pagini04) Reading Vocabulary Question鄭少綸Încă nu există evaluări
- Weirdo. How Misunderstood Human Beings Become MisfitsDocument2 paginiWeirdo. How Misunderstood Human Beings Become Misfitsandreas.hoferÎncă nu există evaluări
- Train The Trainer 1103Document26 paginiTrain The Trainer 1103Andrei Zaha100% (1)
- Jurnal Inter 2Document20 paginiJurnal Inter 2Alissa TextileÎncă nu există evaluări
- Artificial Intelligence by DiproDocument15 paginiArtificial Intelligence by DiproUchchhwas Saha 181-15-10842Încă nu există evaluări
- Docslide - Us Fp601-CyberpreneurshipDocument4 paginiDocslide - Us Fp601-CyberpreneurshipKadem AmirudinÎncă nu există evaluări
- Round and Flat Characters LPDocument4 paginiRound and Flat Characters LPJames Andrew PaddayumanÎncă nu există evaluări
- Facilitating Learner Centered Teaching Module 19 26Document72 paginiFacilitating Learner Centered Teaching Module 19 26Katherine Anne Munar-GuralÎncă nu există evaluări
- Cala 1 IctDocument8 paginiCala 1 IctaddyÎncă nu există evaluări
- AECS Lab ManualDocument69 paginiAECS Lab ManuallemuelgeorgeÎncă nu există evaluări
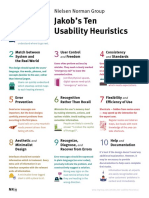
- Heuristic Summary1 CompressedDocument1 paginăHeuristic Summary1 CompressedJaime RodriguezÎncă nu există evaluări
- Project Management Interview Questions and AnswersDocument2 paginiProject Management Interview Questions and AnswersStewart Bimbola Obisesan100% (1)