S-ar putea să vă placă și
- Epi & StatisticsDocument135 paginiEpi & StatisticsFatma AlSayeghÎncă nu există evaluări
- Diagnostic Test DesignDocument30 paginiDiagnostic Test DesignDika Gita PratamaÎncă nu există evaluări
- Screening of DiseasesDocument50 paginiScreening of Diseasesravi_rohilla100% (1)
- Evidence Based Medicine: Kiki Lukman, Bagian Bedah Fakultas Kedokteran UNPAD/ RS DR Hasan Sadikin BandungDocument70 paginiEvidence Based Medicine: Kiki Lukman, Bagian Bedah Fakultas Kedokteran UNPAD/ RS DR Hasan Sadikin BandungOby BedahÎncă nu există evaluări
- Diagnostic TestDocument26 paginiDiagnostic Testefmed2001Încă nu există evaluări
- Protokol Critical ApraisalDocument16 paginiProtokol Critical ApraisalMustika ayu lestariÎncă nu există evaluări
- Study of Diagnostic Test - Mirawati SudiroDocument32 paginiStudy of Diagnostic Test - Mirawati SudiroAVG2011Încă nu există evaluări
- Critical Appraisal: On Article of Diagnostic Test (EBM-Diagnostic)Document28 paginiCritical Appraisal: On Article of Diagnostic Test (EBM-Diagnostic)Giovan GaulÎncă nu există evaluări
- Lecture 8 and 9 Slides DiagnosisDocument35 paginiLecture 8 and 9 Slides DiagnosisJustDen09100% (1)
- Diagnosis: Research Methods Dent 313Document35 paginiDiagnosis: Research Methods Dent 313Rmz StudyÎncă nu există evaluări
- Screening: Department of Public Health Medical School, University of PécsDocument38 paginiScreening: Department of Public Health Medical School, University of PécsESSA GHAZWANI100% (1)
- QC Delta PV PPT Student 09Document8 paginiQC Delta PV PPT Student 09Susianna RismandaÎncă nu există evaluări
- Clinical Decision MakingDocument32 paginiClinical Decision MakingMUGISHA GratienÎncă nu există evaluări
- Screening TestDocument22 paginiScreening TestRabea DiaÎncă nu există evaluări
- Quality Control in Clinical Biochemistry BMLTDocument56 paginiQuality Control in Clinical Biochemistry BMLTSelim JaforÎncă nu există evaluări
- Probabilities in Clinical Medicine: Mohammad Saifur Rohman, Md. PHDDocument41 paginiProbabilities in Clinical Medicine: Mohammad Saifur Rohman, Md. PHDerlisaÎncă nu există evaluări
- Screening - DR Heba MahmoudDocument45 paginiScreening - DR Heba MahmoudMerna IbrahimÎncă nu există evaluări
- Lecture 2 Cpms16-ScreeningDocument40 paginiLecture 2 Cpms16-Screeningapi-263590842Încă nu există evaluări
- Practical Work CA On DX 2012Document26 paginiPractical Work CA On DX 2012Nurul Aulia AbdullahÎncă nu există evaluări
- Westgard1983 - Power CurvesDocument8 paginiWestgard1983 - Power CurvesAnderson CarvalhoÎncă nu există evaluări
- Decision Analysis: Matthew Scotch, PHD, MPHDocument29 paginiDecision Analysis: Matthew Scotch, PHD, MPHPedroMartinsÎncă nu există evaluări
- Quality ControlDocument65 paginiQuality ControlKirsten ValenzuelaÎncă nu există evaluări
- Epi Lec 5Document40 paginiEpi Lec 5Dr. Mahbub Alam MahfuzÎncă nu există evaluări
- Week 6-MCQ in EBP-1Document36 paginiWeek 6-MCQ in EBP-1Hasan KhawaldehÎncă nu există evaluări
- Week 6-MCQ in EBP-1Document36 paginiWeek 6-MCQ in EBP-1Geeta SureshÎncă nu există evaluări
- Conditional Probability and Medical TestsDocument20 paginiConditional Probability and Medical TestsRuslan MalovanyyÎncă nu există evaluări
- Diagnostic Studies PEBHC Workshop December 2015Document77 paginiDiagnostic Studies PEBHC Workshop December 2015Nursyamsi AhmadÎncă nu există evaluări
- 4 - Clinical EpidemiologyDocument8 pagini4 - Clinical EpidemiologyDiana Mitrea100% (1)
- Jarir Atthobari - Clinical TrialDocument38 paginiJarir Atthobari - Clinical TrialLilian KusumaÎncă nu există evaluări
- Introduction To Laboratory Medicine (Clinical Laboratory) : Dr. Dr. Tinny Rasjad SPPK (K)Document43 paginiIntroduction To Laboratory Medicine (Clinical Laboratory) : Dr. Dr. Tinny Rasjad SPPK (K)hendra2darmawanÎncă nu există evaluări
- Screening: To Sort Out Apparently Well Persons Who Probably Have A Disease From Those Who Probably Do Not."Document24 paginiScreening: To Sort Out Apparently Well Persons Who Probably Have A Disease From Those Who Probably Do Not."Munir AkhtarÎncă nu există evaluări
- 29 Sep 2023principles and Predictive Value of ScreeningDocument29 pagini29 Sep 2023principles and Predictive Value of Screening1.barron.whiteÎncă nu există evaluări
- Screening: Owais Raza - PHD Epidemiology - Tehran University of Medical SciencesDocument35 paginiScreening: Owais Raza - PHD Epidemiology - Tehran University of Medical Sciencespaperpin27100% (1)
- Summary of Diagnostic Test Accuracy For BR PDFDocument33 paginiSummary of Diagnostic Test Accuracy For BR PDFOlfat ashrafÎncă nu există evaluări
- Screening Test (Adv) : Rizwanul Karim NipsomDocument37 paginiScreening Test (Adv) : Rizwanul Karim NipsomRizwan ShameemÎncă nu există evaluări
- Evidence Based Medicine: Tugas MkduDocument6 paginiEvidence Based Medicine: Tugas MkduPutri Dwi KartiniÎncă nu există evaluări
- EBM TerapiDocument23 paginiEBM TerapiArum Ardisa RiniÎncă nu există evaluări
- Diagnostic and Prognostic Worksheet by DR Muhammad Febriandi Djunaidi Prodi Ilmu BedahDocument8 paginiDiagnostic and Prognostic Worksheet by DR Muhammad Febriandi Djunaidi Prodi Ilmu BedahMuhammad FebriandiÎncă nu există evaluări
- ENG - Epidemiology Biostatistics IMGDocument8 paginiENG - Epidemiology Biostatistics IMGManivanh AvalosÎncă nu există evaluări
- Quality Assurance in Hematology Group 11Document51 paginiQuality Assurance in Hematology Group 11Mandy A. DelfinÎncă nu există evaluări
- Quality Assurance in Hemat LabsDocument38 paginiQuality Assurance in Hemat LabsSmriti Dwivedi SharmaÎncă nu există evaluări
- MANI Quality Control in Hematology AnalysersDocument65 paginiMANI Quality Control in Hematology Analyserscandiddreams100% (1)
- Student Worksheet - CA DX - 221122Document5 paginiStudent Worksheet - CA DX - 221122MuhammadDzikriAuliaÎncă nu există evaluări
- Disease ScreeningDocument37 paginiDisease Screeningmwambungup100% (1)
- Lecture5 June15 05Document45 paginiLecture5 June15 05Wuri Kusuma AtmajaÎncă nu există evaluări
- Screening - Master - 2022Document57 paginiScreening - Master - 2022Kanwal KhanÎncă nu există evaluări
- Critical Appraisal of Articles About Diagnostic TestsDocument43 paginiCritical Appraisal of Articles About Diagnostic TestshardianÎncă nu există evaluări
- Screening TestsDocument35 paginiScreening Testsapi-3699330Încă nu există evaluări
- EBM, Design Study, Quantifying RiskDocument71 paginiEBM, Design Study, Quantifying Riskseptian kristyanaÎncă nu există evaluări
- Critical Appraisal Cross Sectional Case ControlDocument76 paginiCritical Appraisal Cross Sectional Case ControlAndita SyabanaÎncă nu există evaluări
- Update To The 2009 AMP Molecular Diagnostic Assay Validation White PaperDocument11 paginiUpdate To The 2009 AMP Molecular Diagnostic Assay Validation White PaperHuỳnh ChâuÎncă nu există evaluări
- Study Desien - by Tahani AlghamdiDocument41 paginiStudy Desien - by Tahani AlghamdiMian. Shoaib.Încă nu există evaluări
- Bio Statistics Hand OutDocument11 paginiBio Statistics Hand OutaymÎncă nu există evaluări
- Chapter 8Document26 paginiChapter 8Nathnael GebÎncă nu există evaluări
- Quality Control: Lucila B. Rabuco, PHDDocument47 paginiQuality Control: Lucila B. Rabuco, PHDChito PermejoÎncă nu există evaluări
- Journalclubjan 2015Document25 paginiJournalclubjan 2015api-277377339Încă nu există evaluări
- L 5 - Reference RangeDocument32 paginiL 5 - Reference RangehayatkuwaityÎncă nu există evaluări
- Interpretation of Diagnostic Screening TestsDocument33 paginiInterpretation of Diagnostic Screening TestsAMELIA CAROLINA HERRERA BRICEÑOÎncă nu există evaluări
- Nuclear Medicine Clinical Procedures for TechnologistsDe la EverandNuclear Medicine Clinical Procedures for TechnologistsÎncă nu există evaluări
- Elements Of Clinical Study Design, Biostatistics & ResearchDe la EverandElements Of Clinical Study Design, Biostatistics & ResearchÎncă nu există evaluări
- Iggy Med Surg Test Bank Chapter 007Document10 paginiIggy Med Surg Test Bank Chapter 007Tracy Bartell100% (5)
- Endometrial HyperplasiaDocument11 paginiEndometrial HyperplasiarinieeeÎncă nu există evaluări
- Gastroesophageal Reflux DiseaseDocument9 paginiGastroesophageal Reflux DiseaseNicole Tupayachi ArceÎncă nu există evaluări
- Dha 022019 PDFDocument20 paginiDha 022019 PDFDrNishchitha K100% (2)
- What Is ThalassemiaDocument2 paginiWhat Is ThalassemiaFatima Azzahra Khairul AnuarÎncă nu există evaluări
- NCP For Laryngeal CancerDocument5 paginiNCP For Laryngeal CancerMădălina PinciucÎncă nu există evaluări
- Department of Oral Periodontology: Topic: Free Gingival GraftDocument1 paginăDepartment of Oral Periodontology: Topic: Free Gingival GraftTenzin WangyalÎncă nu există evaluări
- Medical ReportDocument5 paginiMedical ReportRuthdel KazumiÎncă nu există evaluări
- A Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESDocument57 paginiA Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESLane Mae Magpatoc NoerrotÎncă nu există evaluări
- Medication, Toxic, and Vitamin-Related NeuropathiesDocument22 paginiMedication, Toxic, and Vitamin-Related Neuropathiessatyagraha84Încă nu există evaluări
- Total Patient Care Nursing or Case Method NursingDocument3 paginiTotal Patient Care Nursing or Case Method Nursingkint manlangitÎncă nu există evaluări
- For Website All Questions PDFDocument26 paginiFor Website All Questions PDFAyyaz HussainÎncă nu există evaluări
- OpicaponeDocument4 paginiOpicaponeAnonymous a6UCbaJÎncă nu există evaluări
- Director Emergency Medical Services in Nashville TN Resume Steve FustonDocument2 paginiDirector Emergency Medical Services in Nashville TN Resume Steve FustonSteveFustonÎncă nu există evaluări
- 129 Accommodative EsotropiaDocument6 pagini129 Accommodative EsotropiakarenafiafiÎncă nu există evaluări
- Annotated BibliographyDocument2 paginiAnnotated Bibliographyapi-237172063Încă nu există evaluări
- In-Patient Claim Form - ConventionalDocument2 paginiIn-Patient Claim Form - ConventionalAbdul Qayyum Sipra Madduki50% (2)
- ENT 2014 SovedDocument7 paginiENT 2014 SovedHasnat HussainÎncă nu există evaluări
- Baromtric (89 Pages)Document89 paginiBaromtric (89 Pages)jahangirealamÎncă nu există evaluări
- Improving Patient and Worker SafetyDocument171 paginiImproving Patient and Worker SafetylaggantigganÎncă nu există evaluări
- Bronchial Asthma SeminarDocument64 paginiBronchial Asthma SeminarShidevÎncă nu există evaluări
- As Far As Possible - en ISO 14971Document19 paginiAs Far As Possible - en ISO 14971Kanwal Jit Singh100% (1)
- Analyzing A Leader EssayDocument6 paginiAnalyzing A Leader Essayapi-253792021Încă nu există evaluări
- Granny Storm Crow's List Jan 2014 ConditionsDocument750 paginiGranny Storm Crow's List Jan 2014 ConditionsElectroPig Von FökkenGrüüvenÎncă nu există evaluări
- FullDocument59 paginiFullJyotiÎncă nu există evaluări
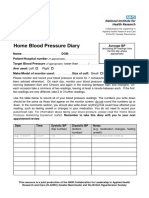
- Home Blood Pressure DiaryDocument2 paginiHome Blood Pressure DiaryCherieÎncă nu există evaluări
- USG Efusi Pleura PDFDocument7 paginiUSG Efusi Pleura PDFEnvhy AmaliaÎncă nu există evaluări
- SMA Advanced Sports Taping Presentation DSR Handouts PDFDocument4 paginiSMA Advanced Sports Taping Presentation DSR Handouts PDFHamada Said AliÎncă nu există evaluări
- Hospital Design GuidelinesDocument33 paginiHospital Design GuidelinesRohit Gupta100% (3)
- Thesis PoDocument5 paginiThesis PoJane SandovalÎncă nu există evaluări