S-ar putea să vă placă și
- DR Bradley Nelson - Rapid Results Start Up GuideDocument9 paginiDR Bradley Nelson - Rapid Results Start Up Guideemily turner100% (1)
- Nov 2017 Infantile Spasms WebinarDocument22 paginiNov 2017 Infantile Spasms WebinartetiÎncă nu există evaluări
- Ge Healthcare Oec 9900 Elite Equiptment SpecificationsDocument8 paginiGe Healthcare Oec 9900 Elite Equiptment SpecificationsAhmed Torky100% (1)
- Case Based Pediatrics For Medical Students and ResidentsDocument6 paginiCase Based Pediatrics For Medical Students and Residentssantosaerwin6591100% (1)
- Febrile SeizureDocument8 paginiFebrile Seizureanon_944507650Încă nu există evaluări
- Cyclic Vomiting SyndromeDocument17 paginiCyclic Vomiting Syndromeminerva_stanciuÎncă nu există evaluări
- DOH Calendar of ActivitiesDocument4 paginiDOH Calendar of ActivitiesArlene Cerdeña SalcedaÎncă nu există evaluări
- Febrile Seizures: Clinical Practice Guideline For The Long-Term Management of The Child With Simple Febrile SeizuresDocument8 paginiFebrile Seizures: Clinical Practice Guideline For The Long-Term Management of The Child With Simple Febrile SeizuresRichel Edwin Theofili PattikawaÎncă nu există evaluări
- Technical Report: Treatment of The Child With Simple Febrile SeizuresDocument59 paginiTechnical Report: Treatment of The Child With Simple Febrile SeizuresCiara May SeringÎncă nu există evaluări
- Pediatrics 1996 769 72Document6 paginiPediatrics 1996 769 72Bincar PardomuanÎncă nu există evaluări
- Presentasi Jurnal Kejang DemamDocument21 paginiPresentasi Jurnal Kejang DemamSeptiana WahyuÎncă nu există evaluări
- Evaluasi Anak Dengan Kejang DemamDocument4 paginiEvaluasi Anak Dengan Kejang DemamdavidÎncă nu există evaluări
- Acn30001 0171 PDFDocument9 paginiAcn30001 0171 PDFKoas PatoÎncă nu există evaluări
- Epilepsy: EssentialsDocument3 paginiEpilepsy: Essentialshannah_pharmÎncă nu există evaluări
- Author: Section Editor: Deputy EditorDocument26 paginiAuthor: Section Editor: Deputy EditorBùi Công MinhÎncă nu există evaluări
- Clinical Evidence ConciseDocument4 paginiClinical Evidence ConciseisxyÎncă nu există evaluări
- BFCDocument7 paginiBFCKalvinKonOjalesStrangerÎncă nu există evaluări
- Febrile Seizures: Definition and ClassificationDocument3 paginiFebrile Seizures: Definition and ClassificationArmin AbasÎncă nu există evaluări
- Journjkljal 2 PDFDocument9 paginiJournjkljal 2 PDFAan AchmadÎncă nu există evaluări
- Management of Febrile Seizures in Children: Khawaja Tahir Mahmood, Tooba Fareed, Rabia TabbasumDocument5 paginiManagement of Febrile Seizures in Children: Khawaja Tahir Mahmood, Tooba Fareed, Rabia TabbasumrizkianaÎncă nu există evaluări
- Sharief F 2011Document14 paginiSharief F 2011wiwiÎncă nu există evaluări
- Guideline Summary NGC-9469: RecommendationsDocument6 paginiGuideline Summary NGC-9469: RecommendationsIbrahim MachmudÎncă nu există evaluări
- Epilepsy treatment-UpToDateDocument29 paginiEpilepsy treatment-UpToDateclarestaÎncă nu există evaluări
- Absence Seizures in Children: QuestionsDocument7 paginiAbsence Seizures in Children: QuestionsAliss OñaÎncă nu există evaluări
- 100 Case Studies in Pathophysiology-532hlm (Warna Hanya Cover)Document11 pagini100 Case Studies in Pathophysiology-532hlm (Warna Hanya Cover)Haymanot AnimutÎncă nu există evaluări
- Neonatal Seizures Semfetneo2013press-1Document7 paginiNeonatal Seizures Semfetneo2013press-1Vianney Olvera SánchezÎncă nu există evaluări
- Management of Febrile SeizuresDocument9 paginiManagement of Febrile SeizuresLi FaungÎncă nu există evaluări
- Febrile SeizureDocument6 paginiFebrile SeizurepipimseptianaÎncă nu există evaluări
- Simple Versus Complex Febrile SeizureDocument18 paginiSimple Versus Complex Febrile SeizurePiet SeLoesindÎncă nu există evaluări
- Evaluation and Management of Drug Resistant Epilepsy in ChildrenDocument10 paginiEvaluation and Management of Drug Resistant Epilepsy in ChildrenAzizah HalidÎncă nu există evaluări
- The Treatment of Migraine Headaches in Children and AdolescentsDocument11 paginiThe Treatment of Migraine Headaches in Children and Adolescentsdo leeÎncă nu există evaluări
- Risk Factors of Recurrence of Febrile Seizures in Children in A Tertiary Care Hospital in Kanpur - A One Year Follow Up StudyDocument7 paginiRisk Factors of Recurrence of Febrile Seizures in Children in A Tertiary Care Hospital in Kanpur - A One Year Follow Up StudyFarra PattipawaeÎncă nu există evaluări
- 10.14 Other Epilepsy Syndromes: The Epilepsies Partial Pharmacological Update of Clinical Guideline 20 443Document4 pagini10.14 Other Epilepsy Syndromes: The Epilepsies Partial Pharmacological Update of Clinical Guideline 20 443foxysformeÎncă nu există evaluări
- NewbornEmergenices2006 PDFDocument16 paginiNewbornEmergenices2006 PDFRana SalemÎncă nu există evaluări
- I. Inroduction Benign Febrile Convulsion: Seizures or Convulsions Are Sudden, Abnormal Electrical Discharges FromDocument8 paginiI. Inroduction Benign Febrile Convulsion: Seizures or Convulsions Are Sudden, Abnormal Electrical Discharges FromJd SantosÎncă nu există evaluări
- Case Vignette. EpilepsyDocument8 paginiCase Vignette. EpilepsyAizel ManiagoÎncă nu există evaluări
- Predictors of Intractable Epilepsy in Childhood: Case-Control StudyDocument7 paginiPredictors of Intractable Epilepsy in Childhood: Case-Control StudyArdiya OktamaÎncă nu există evaluări
- Seizures in Children JULIO 2020Document29 paginiSeizures in Children JULIO 2020Elizabeth HendersonÎncă nu există evaluări
- Neonatal Epilepsy SyndromesDocument22 paginiNeonatal Epilepsy SyndromesJUAN CAMILO LANDAZURIÎncă nu există evaluări
- Sloan Szse Acep 2005 PedsDocument8 paginiSloan Szse Acep 2005 Pedsstrawberry pieÎncă nu există evaluări
- Fernandez, John Michael BSN403 Group 10: I. Clinical QuestionDocument5 paginiFernandez, John Michael BSN403 Group 10: I. Clinical QuestionJohn Michael FernandezÎncă nu există evaluări
- Generalized Convulsive Status Epilepticus in Adults and Children Treatment Guidelines and ProtocolsReviewDocument14 paginiGeneralized Convulsive Status Epilepticus in Adults and Children Treatment Guidelines and ProtocolsReviewAribeth PeñalozaÎncă nu există evaluări
- New Antiepileptic Agents: Literature ReviewDocument5 paginiNew Antiepileptic Agents: Literature ReviewYenny mardiatyÎncă nu există evaluări
- 72 FullDocument1 pagină72 FullalfredoibcÎncă nu există evaluări
- Clinical Management of Seizures in Newborns: Diagnosis and TreatmentDocument10 paginiClinical Management of Seizures in Newborns: Diagnosis and TreatmentfitriÎncă nu există evaluări
- Seizures in Children - Pediatric in Review 2020Document29 paginiSeizures in Children - Pediatric in Review 2020Apple B RaiwaaÎncă nu există evaluări
- Drugs in Context Volume 7 Issue 2018 (Doi 10.7573 - Dic.212536) Leung, Alexander KC Hon, Kam Lun Leung, Theresa NH - Febrile Seizures - An OverviewDocument12 paginiDrugs in Context Volume 7 Issue 2018 (Doi 10.7573 - Dic.212536) Leung, Alexander KC Hon, Kam Lun Leung, Theresa NH - Febrile Seizures - An OverviewAlwin Ardiansyah PulunganÎncă nu există evaluări
- C C C ! "##$%& ' $#+ ,-C " % .# .# " / 1 !% ! 23 "% 23 ! C % !Document4 paginiC C C ! "##$%& ' $#+ ,-C " % .# .# " / 1 !% ! 23 "% 23 ! C % !ejkohÎncă nu există evaluări
- Unveiling of Cannabidiol in The Treatment of Rare Childhood Epilepsies: Dravet and Lennox Gastaut SyndromesDocument14 paginiUnveiling of Cannabidiol in The Treatment of Rare Childhood Epilepsies: Dravet and Lennox Gastaut SyndromesMediterr J Pharm Pharm SciÎncă nu există evaluări
- Febrile SeizuresDocument18 paginiFebrile Seizureskara_korum100% (1)
- DMCN 14015Document10 paginiDMCN 14015Anida HasnaÎncă nu există evaluări
- Evidence Based Nursing: Batch 2011Document7 paginiEvidence Based Nursing: Batch 2011Eimhie Lee CasiÎncă nu există evaluări
- Laporan Kasus Tonsilofaringitis AkutDocument8 paginiLaporan Kasus Tonsilofaringitis AkutAvhindAvhindÎncă nu există evaluări
- Practice Essentials: Simple Febrile SeizureDocument7 paginiPractice Essentials: Simple Febrile SeizureRebeca SpataruÎncă nu există evaluări
- Epilepsy Research Paper PDFDocument8 paginiEpilepsy Research Paper PDFyscgudvnd100% (1)
- Research Article: ObjectiveDocument5 paginiResearch Article: ObjectiveFerdina NidyasariÎncă nu există evaluări
- Febrile Seizures: Jithangi WanigasingheDocument5 paginiFebrile Seizures: Jithangi WanigasingheNadya ErlianieÎncă nu există evaluări
- Approach To Refractory Childhood SeizuresDocument10 paginiApproach To Refractory Childhood SeizureskholisahnasutionÎncă nu există evaluări
- Florida Heart CPR Febrile Seizures 1 Hour: ObjectivesDocument5 paginiFlorida Heart CPR Febrile Seizures 1 Hour: ObjectivesKamelÎncă nu există evaluări
- Waiting Time EpilepsyDocument7 paginiWaiting Time EpilepsyFlavia Angelina SatopohÎncă nu există evaluări
- Epilepsy Research Paper ConclusionDocument7 paginiEpilepsy Research Paper Conclusionzpyrufrif100% (1)
- A Practical Guide to Supporting People with EpilepsyDe la EverandA Practical Guide to Supporting People with EpilepsyÎncă nu există evaluări
- 21.1 - Relaciones de Psicoterapia Que Funcionan III - NorcrossDocument13 pagini21.1 - Relaciones de Psicoterapia Que Funcionan III - NorcrossJocelyn G. García R.Încă nu există evaluări
- Drug Medication ScriptDocument3 paginiDrug Medication Scriptadrian nakilaÎncă nu există evaluări
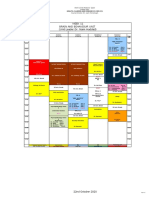
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Document1 paginăWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3Încă nu există evaluări
- Guidance For Provision of A Pharmacist Only Medicine LevonorgestrelDocument3 paginiGuidance For Provision of A Pharmacist Only Medicine LevonorgestrelYusri KardoÎncă nu există evaluări
- IDA Membership FormDocument3 paginiIDA Membership FormAbhijit LeleÎncă nu există evaluări
- Theoretical Framework: Linder-Pelz, S. (1982) : Toward A Theory of Patient Satisfaction. Social Science andDocument7 paginiTheoretical Framework: Linder-Pelz, S. (1982) : Toward A Theory of Patient Satisfaction. Social Science andJoanna EdenÎncă nu există evaluări
- Threshold Elements - Voluntariness and CapacityDocument18 paginiThreshold Elements - Voluntariness and Capacityapi-136237609Încă nu există evaluări
- Submitted By:: Marietta C. Lacsina, Ed.DDocument5 paginiSubmitted By:: Marietta C. Lacsina, Ed.DKathleen Hipolito YunÎncă nu există evaluări
- Is The Smile Line A Valid Parameter For Esthetic Evaluation A Systematic Literature ReviewDocument14 paginiIs The Smile Line A Valid Parameter For Esthetic Evaluation A Systematic Literature Reviewmaroun ghalebÎncă nu există evaluări
- 70 DBEFC7 D 01Document44 pagini70 DBEFC7 D 01ajithnair1Încă nu există evaluări
- Learning Plan Evaluation TemplateDocument10 paginiLearning Plan Evaluation TemplatemylifeascharlyÎncă nu există evaluări
- Global Medicines Use in 2020: Outlook and ImplicationsDocument47 paginiGlobal Medicines Use in 2020: Outlook and Implicationssobrina25355Încă nu există evaluări
- Government of KeralaDocument9 paginiGovernment of KeralaMubashirÎncă nu există evaluări
- Talib Hashmi's ResumeDocument1 paginăTalib Hashmi's ResumeRahul TripathiÎncă nu există evaluări
- PRF CGF AFG PRP PRGF and Sticky Bone or I-PRF - Bauer SmilesDocument1 paginăPRF CGF AFG PRP PRGF and Sticky Bone or I-PRF - Bauer SmilesArmareality ArmarealityÎncă nu există evaluări
- Shadowing Journal 1Document3 paginiShadowing Journal 1api-542121618Încă nu există evaluări
- Scope of Nle1113Document379 paginiScope of Nle1113ericÎncă nu există evaluări
- Analysis, Design, Development & Testing MethodologyDocument47 paginiAnalysis, Design, Development & Testing Methodologyyashbhatt9013Încă nu există evaluări
- Tamayo - History of Psychiatric NursingDocument1 paginăTamayo - History of Psychiatric NursingVictoria Castillo TamayoÎncă nu există evaluări
- Rps - Professional Standards For Hospital Pharmacy PDFDocument33 paginiRps - Professional Standards For Hospital Pharmacy PDFDrAmit VermaÎncă nu există evaluări
- Icd 10Document4 paginiIcd 10Radhika ShahÎncă nu există evaluări
- Hayya Moph QLMDocument4 paginiHayya Moph QLMrrthamadÎncă nu există evaluări
- Bacud, Parick Jayson C.Document4 paginiBacud, Parick Jayson C.Patrick Jayson BacudÎncă nu există evaluări
- The Aborigines of AustraliaDocument13 paginiThe Aborigines of AustraliaVincentÎncă nu există evaluări
- p214 PDFDocument3 paginip214 PDFNinaÎncă nu există evaluări
- Jerarquización de La Evidencia, Niveles y Grados de Recomendación PDFDocument14 paginiJerarquización de La Evidencia, Niveles y Grados de Recomendación PDFVictoria Rojas AlvearÎncă nu există evaluări
- Brochure SPC2023Document3 paginiBrochure SPC2023Edwin KurniawanÎncă nu există evaluări